Cheong Taul, Ahn Jungmo, Kim Yun Seop, Pai Hyunjoo, Kim Bongyoung
Department of Economics, Indiana University Purdue University Indianapolis, Indianapolis, IN, USA.
School of Medicine, Hanyang University College of Medicine, Seoul, Korea.
Infect Chemother. 2022 Sep;54(3):456-469. doi: 10.3947/ic.2022.0057. Epub 2022 Jul 27.
The proportion of antimicrobial-resistant as a causative pathogen of community-acquired acute pyelonephritis (APN) has been increasing. The aim of this study was to quantitatively evaluate the impact of antimicrobial resistance on medical costs and length of hospital stay for the treatment of APN.
A single-center retrospective cohort study was conducted between January 2018 and December 2019. All hospitalized patients aged ≥19 years who were diagnosed with community-acquired APN were recruited, and those diagnosed with as a causative pathogen were included. Log-linear regression analysis was performed to determine the risk factors for medical costs and length of hospital stay.
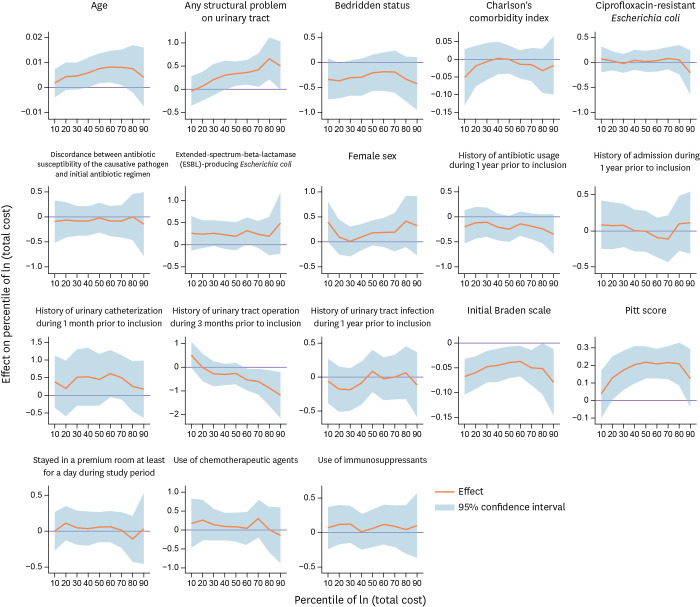
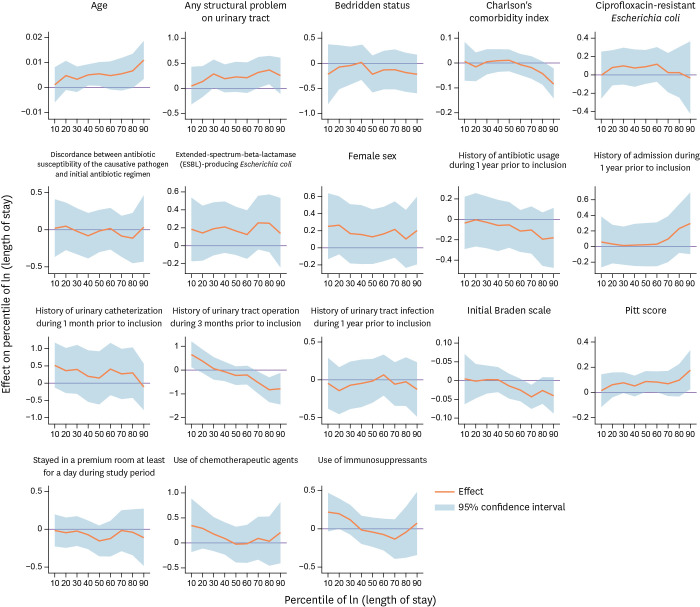
A total of 241 patients participated in this study. Of these, 75 (31.1%) and 87 (36.1%) had extended-spectrum beta-lactamase (ESBL)-producing pathogens and ciprofloxacin-resistant pathogens as the causative pathogen, respectively. Based on the log-linear regression model, ESBL-producing is a causative pathogen that is, on average, 27.0%, or United States Dollar (USD) 1,211 ( = 0.026) more expensive than non-ESBL-producing . A patient who is a year older would incur USD 23 ( = 0.040) more, those having any structural problems in the urinary tract would incur USD 1,231 ( = 0.015) more, and those with a unit increase in the Pitt bacteremia score would incur USD 767 ( <0.001) more, with all other variables constant. Having a case in which ESBL-producing is a causative pathogen would explain staying 22.0% longer or 2 more days ( = 0.050) in the hospital than non-ESBL-producing . A patient who is 10 years older would, on average, would have to stay for half a day longer ( = 0.045). Any structural problems in the urinary tract explain a longer stay (2.4 days longer; = 0.032), and moving from 0 to 5 on the Pitt bacteremia score would explain four more days ( = 0.038) in the hospital.
Patients with community-acquired APN with ESBL-producing Enterobacteriale as the causative pathogen would incur, on average, 27.0% higher medical costs and 22.0% longer hospitalization days than patients detected with non-ESBL-producing pathogens.
作为社区获得性急性肾盂肾炎(APN)致病病原体的抗菌药物耐药菌比例一直在上升。本研究的目的是定量评估抗菌药物耐药性对APN治疗的医疗费用和住院时间的影响。
于2018年1月至2019年12月进行了一项单中心回顾性队列研究。纳入所有年龄≥19岁、诊断为社区获得性APN的住院患者,以及那些诊断为以[具体病原体]作为致病病原体的患者。进行对数线性回归分析以确定医疗费用和住院时间的危险因素。
共有241名患者参与本研究。其中,分别有75例(31.1%)和87例(36.1%)的致病病原体为产超广谱β-内酰胺酶(ESBL)的病原体和对环丙沙星耐药的病原体。基于对数线性回归模型,产ESBL的[具体病原体]作为致病病原体时,平均费用比不产ESBL的[具体病原体]高出27.0%,即1211美元(P = 0.026)。年龄每增加一岁,患者费用会增加23美元(P = 0.040);尿路有任何结构问题的患者费用会增加1231美元(P = 0.015);Pitt菌血症评分每增加一个单位,费用会增加767美元(P<0.001),其他变量保持不变。以产ESBL的[具体病原体]作为致病病原体的患者,住院时间比不产ESBL的患者长22.0%,即多2天(P = 0.050)。年龄增加10岁的患者,平均住院时间会多半天(P = 0.045)。尿路的任何结构问题会导致住院时间延长(延长2.4天;P = 0.032),Pitt菌血症评分从0增加到5会导致住院时间多4天(P = 0.038)。
以产ESBL的肠杆菌科细菌作为致病病原体的社区获得性APN患者,平均医疗费用比检测到不产ESBL病原体的患者高27.0%,住院天数长22.0%。