Melbourne Advanced Facial Anatomy Course (MAFAC), Australasian Society of Aesthetic Plastic Surgeons (ASAPS), PO Box 592, Toorak, VIC, 3142, Australia.
Medical Engineering Research Facility (MERF), Queensland University of Technology (QUT), Brisbane, QLD, Australia.
Aesthetic Plast Surg. 2023 Feb;47(1):170-180. doi: 10.1007/s00266-022-02996-3. Epub 2022 Sep 1.
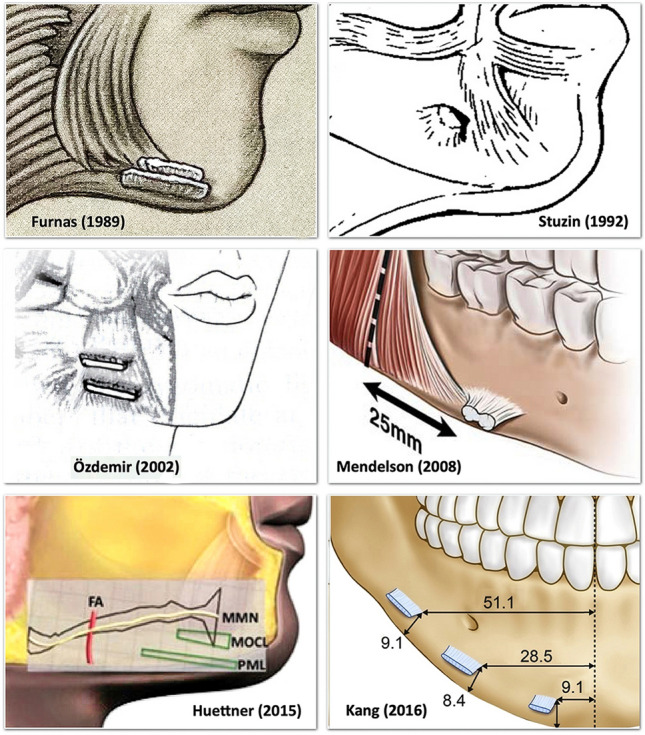
A visible jowl is a reason patients consider lower facial rejuvenation surgery. The anatomical changes that lead to formation of the jowl remain unclear. The aim of this study was to elucidate the anatomy of the jowl, the mandibular ligament and the labiomandibular crease, and their relationship with the marginal mandibular branch of the facial nerve.
Forty-nine cadaver heads were studied (16 embalmed, 33 fresh, mean age 75 years). Following preliminary dissections and macro-sectioning, a series of standardized layered dissections were performed, complemented by histology, sheet plastination and micro-CT.
The jowl forms in the subcutaneous layer where it overlies the posterior part of the mandibular ligament. The mandibular ligament proper exists only in the deep, sub-platysma plane, formed by the combined muscular attachment to the mandible of the specific lower lip depressor muscles and the platysma. The mandibular ligament does not have a definitive subcutaneous component. The labiomandibular crease inferior to the oral commissure marks the posterior extent of the fixed dermal attachment of depressor anguli oris.
Jowls develop as a consequence of aging changes on the functional adaptions of the mouth in humans. To accommodate wide jaw opening with a narrowed commissure requires hypermobility of the tissues overlying the mandible immediately lateral to the level of the oral commissure. This hypermobility over the mandibular attachment of the lower lip depressor muscles occurs entirely in the subcutaneous layer to allow the mandible to move largely independent from the skin. The short, elastic subcutaneous connective tissue, which allows this exceptional mobility without laxity in youth, lengthens with aging, resulting in laxity. The development of subcutaneous and dermal redundancy constitutes the jowl in this location.
"This journal requires that authors assign a level of evidence to each article. For a full description of these Evidence-Based Medicine ratings, please refer to the Table of Contents or the online Instructions to Authors www.springer.com/00266 ."
可见的下颌赘肉是患者考虑进行下面部年轻化手术的原因之一。导致下颌赘肉形成的解剖学变化仍不清楚。本研究旨在阐明下颌赘肉、下颌韧带和唇下颌皱襞的解剖结构及其与面神经下颌缘支的关系。
研究了 49 个头颅标本(16 例防腐,33 例新鲜,平均年龄 75 岁)。在初步解剖和大体解剖后,进行了一系列标准化的分层解剖,并辅以组织学、片状塑化和微 CT。
下颌赘肉位于皮下层,覆盖下颌韧带的后部分。真正的下颌韧带仅存在于深层的、低于颈阔肌的平面,由特定的下唇降肌与下颌的联合肌附着和颈阔肌形成。下颌韧带没有明确的皮下成分。口角下方的唇下颌皱襞标志着降口角肌的皮肤固定附着向后延伸的位置。
下颌赘肉的形成是人类口部功能适应性老化变化的结果。为了适应颌骨张开度增大而口角变窄的需要,需要覆盖下颌的组织在口裂水平的外侧具有高度的可动性。这种覆盖在下唇降肌下颌附着处的可动性完全发生在皮下层,使下颌能够在很大程度上独立于皮肤运动。在年轻人中,允许这种特殊运动而不会松弛的短而有弹性的皮下结缔组织随着年龄的增长而延长,导致松弛。皮下和真皮冗余的发展构成了该部位的下颌赘肉。
证据等级 IV:“本杂志要求作者为每篇文章指定一个证据等级。有关这些循证医学等级的完整描述,请参考目录或在线作者指南 www.springer.com/00266。”