The John Walton Muscular Dystrophy Research Centre, Translational and Clinical Research Institute, Newcastle University and Newcastle Hospitals NHS Foundation Trust, Newcastle upon Tyne, UK.
NMR Laboratory, Neuromuscular Investigation Center, Institute of Myology, Paris, France.
J Cachexia Sarcopenia Muscle. 2022 Dec;13(6):2888-2897. doi: 10.1002/jcsm.13063. Epub 2022 Sep 4.
Water T2 (T2 ) mapping is increasingly being used in muscular dystrophies to assess active muscle damage. It has been suggested as a surrogate outcome measure for clinical trials. Here, we investigated the prognostic utility of T2 to identify changes in muscle function over time in limb girdle muscular dystrophies.
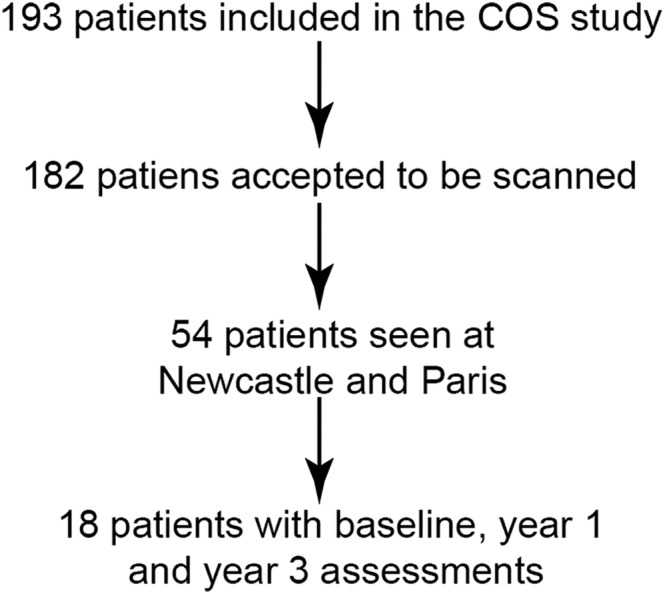
Patients with genetically confirmed dysferlinopathy were assessed as part of the Jain Foundation Clinical Outcomes Study in dysferlinopathy. The cohort included 18 patients from two sites, both equipped with 3-tesla magnetic resonance imaging (MRI) systems from the same vendor. T2 value was defined as higher or lower than the median in each muscle bilaterally. The degree of deterioration on four functional tests over 3 years was assessed in a linear model against covariates of high or low T2 at baseline, age, disease duration, and baseline function.
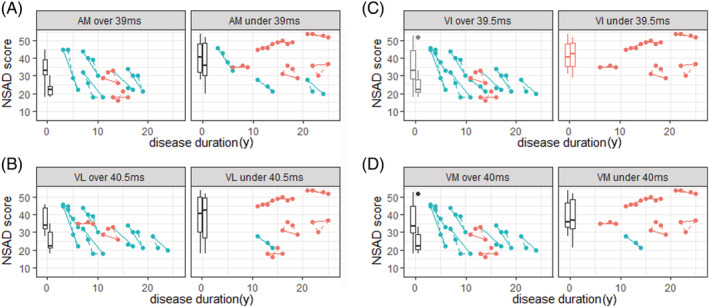
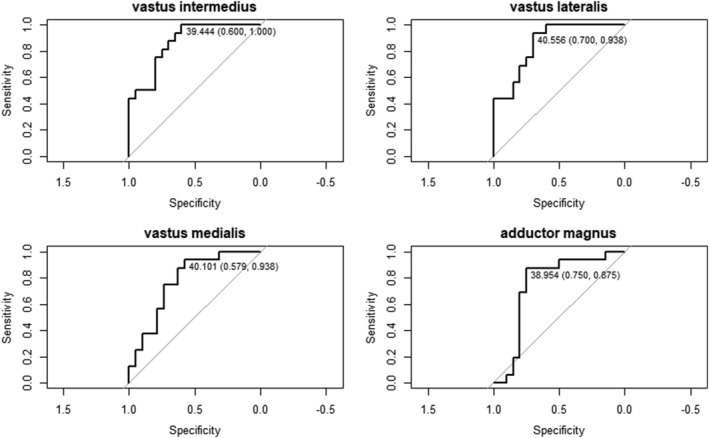
A higher T2 at baseline significantly correlated with a greater decline on functional tests in 21 out of 35 muscles and was never associated with slower decline. Higher baseline T2 in adductor magnus, vastus intermedius, vastus lateralis, and vastus medialis were the most sensitive, being associated bilaterally with greater decline in multiple timed tests. Patients with a higher than median baseline T2 (>40.6 ms) in the right vastus medialis deteriorated 11 points more on the North Star Ambulatory Assessment for Dysferlinopathy and lost an additional 86 m on the 6-min walk than those with a lower T2 (<40.6 ms). Optimum sensitivity and specificity thresholds for predicting decline were 39.0 ms in adductor magnus and vastus intermedius, 40.0 ms in vastus medialis, and 40.5 ms in vastus lateralis from different sites equipped with different MRI systems.
In dysferlinopathy, T2 did not correlate with current functional ability. However, T2 at baseline was higher in patients who worsened more rapidly on functional tests. This suggests that inter-patient differences in functional decline over time may be, in part, explained by different severities of the active muscle damage, assessed by T2 measure at baseline. Significant challenges remain in standardizing T2 values across sites to allow determining globally applicable thresholds. The results from the present work are encouraging and suggest that T2 could be used to improve prognostication, patient selection, and disease modelling for clinical trials.
水 T2(T2)映射在肌肉疾病中越来越多地被用于评估活跃的肌肉损伤。它已被建议作为临床试验的替代终点指标。在这里,我们研究了 T2 的预后效用,以确定肢带型肌肉疾病中肌肉功能随时间的变化。
患有遗传性肌营养不良症的患者被纳入肌营养不良症 Jain 基金会临床结果研究的一部分。该队列包括来自两个地点的 18 名患者,这两个地点都配备了来自同一供应商的 3 特斯拉磁共振成像(MRI)系统。在双侧,T2 值被定义为高于或低于中位数。在 3 年内,使用线性模型根据基线时 T2 值高或低、年龄、疾病持续时间和基线功能等协变量,评估四项功能测试的恶化程度。
基线时 T2 值较高与 35 块肌肉中 21 块肌肉的功能测试下降程度显著相关,且与下降速度较慢无关。基线时内收大肌、股中间肌、股外侧肌和股内侧肌的 T2 值较高与双侧多项定时测试的下降程度更相关。与 T2 值较低的患者相比,基线时右侧股内侧肌 T2 值高于中位数(>40.6ms)的患者在 North Star 肌营养不良症行走评估中恶化了 11 分,在 6 分钟步行测试中损失了额外的 86 米。预测下降的最佳敏感性和特异性阈值为:内收大肌和股中间肌 39.0ms,股内侧肌 40.0ms,股外侧肌 40.5ms,这些阈值来自不同配备不同 MRI 系统的地点。
在肌营养不良症中,T2 与当前的功能能力无关。然而,在功能测试恶化更快的患者中,基线时的 T2 值更高。这表明,随着时间的推移,患者之间功能下降的差异部分可能是由于基线时 T2 测量评估的活跃肌肉损伤的严重程度不同。在不同地点之间标准化 T2 值以确定全球适用的阈值仍然存在重大挑战。目前工作的结果令人鼓舞,表明 T2 可用于改善预后、患者选择和临床试验的疾病建模。