Department of Oncology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China.
Department of Hematology, The First Affiliated Hospital of Wenzhou Medical University, Wenzhou, China.
Front Immunol. 2022 Aug 17;13:963031. doi: 10.3389/fimmu.2022.963031. eCollection 2022.
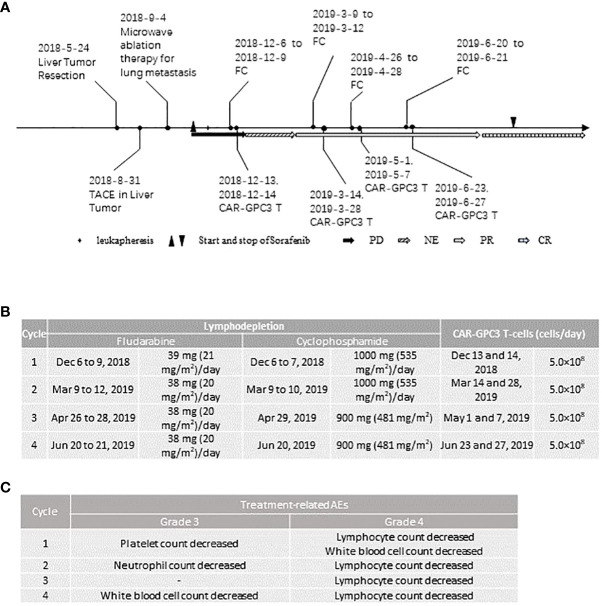
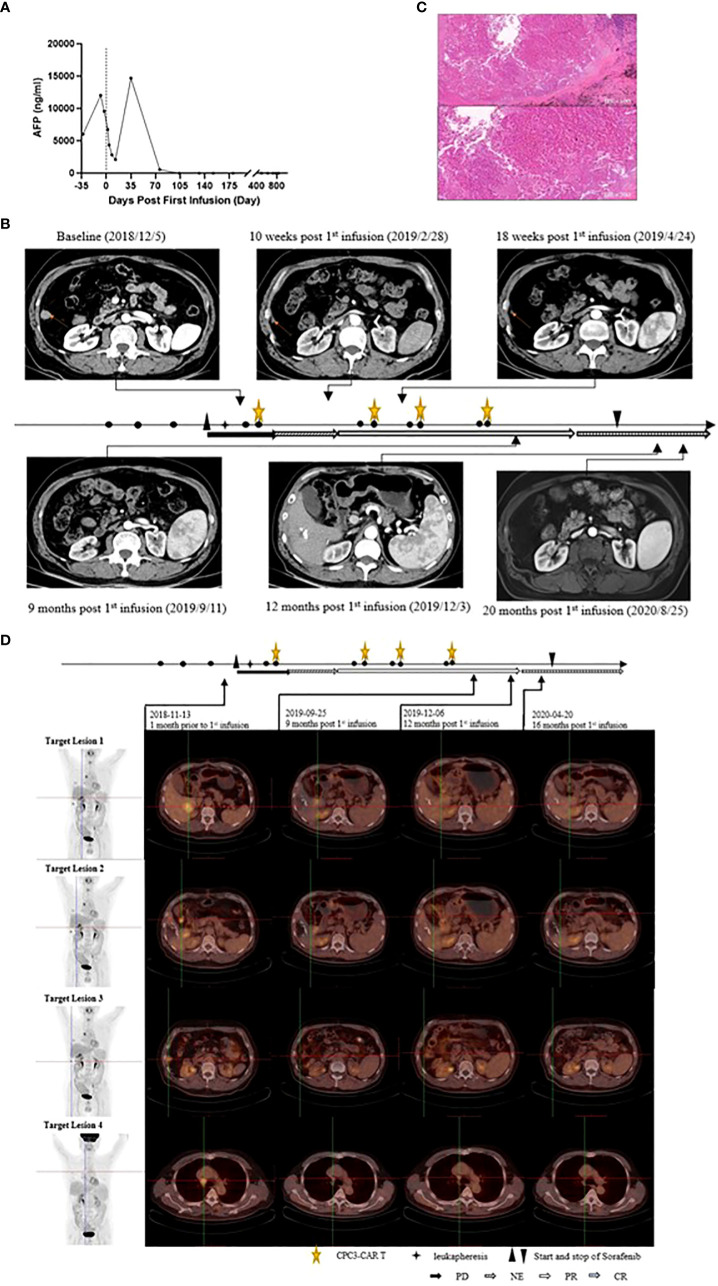
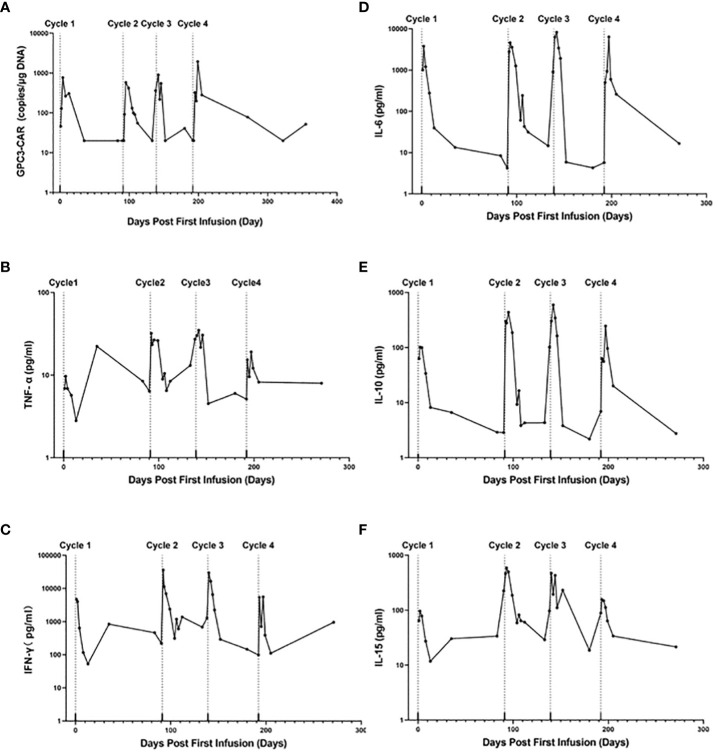
The clinical efficacy of current therapies for Hepatocellular carcinoma (HCC) are unsatisfactory. In recent years, chimeric antigen receptor (CAR) T-cell therapies have been developed for solid tumors including advanced HCC (aHCC), but limited progress has been made. Glypican-3 is a promising immunotherapeutic target for HCC since it is specifically highly expressed in HCC. A previous study indicated that GPC3-targeted CAR T-(CAR-GPC3) cells were well-tolerated and had prolonged survival for HCC patients and that Sorafenib could increase the antitumor activities of CAR-GPC3 T-cells against HCC in mouse models. Here, we report a patient with aHCC who achieved a complete response (CR) and a long survival period after the combination therapy of CAR-GPC3 T-cell plus sorafenib. A 60-year-old Asian male diagnosed with hepatitis B virus (HBV) related HCC developed liver recurrence and lung metastasis after liver tumor resection and trans-arterial chemoembolization therapy. The patient also previously received microwave ablation therapy for lung metastasis. After the enrollment, the patient underwent leukapheresis for CAR-GPC3 T-cells manufacturing. Seven days after leukapheresis, the patient started to receive 400 mg of Sorafenib twice daily. The patient received 4 cycles of CAR-GPC3 T cells (CT011) treatment and each cycle was divided into two infusions. Prior to each cycle of CT011 treatment, lymphodepletion was performed. The lymphodepletion regimen was cyclophosphamide 500 mg/m/day for 2 to 3 days, and fludarabine 20-25 mg/m/day for 3 to 4 days. A total of 4×10 CAR-GPC3 T cells were infused. The CT011 plus Sorafenib combination therapy was well tolerated. All the ≥ grade 3 AEs were hematological toxicities which were deemed an expected event caused by the preconditioning regimen. This patient obtained partial responses from the 3 month and achieved CR in the 12 month after the first cycle of CT011 infusion according to the RECIST1.1 assessment. The tumor had no progression for more than 36 months and maintained the CR status for more than 24 months after the first infusion.
目前治疗肝细胞癌(HCC)的临床疗效并不令人满意。近年来,嵌合抗原受体(CAR)T 细胞疗法已被开发用于包括晚期 HCC(aHCC)在内的实体瘤,但进展有限。磷脂酰聚糖-3 是 HCC 的一个很有前途的免疫治疗靶点,因为它在 HCC 中特异性高度表达。先前的一项研究表明,针对 GPC3 的 CAR T 细胞(CAR-GPC3)对 HCC 患者具有良好的耐受性,并延长了其生存时间,索拉非尼可以提高 CAR-GPC3 T 细胞在小鼠模型中对 HCC 的抗肿瘤活性。在这里,我们报告了一例 aHCC 患者,该患者在接受 CAR-GPC3 T 细胞联合索拉非尼治疗后获得完全缓解(CR)和长期生存。一名 60 岁的亚洲男性,诊断为乙型肝炎病毒(HBV)相关 HCC,在肝肿瘤切除和经动脉化疗栓塞治疗后出现肝复发和肺转移。该患者还曾接受微波消融治疗肺转移。入组后,患者接受白细胞分离术以制造 CAR-GPC3 T 细胞。白细胞分离术后 7 天,患者开始每天服用 400mg 索拉非尼两次。患者接受了 4 个周期的 CAR-GPC3 T 细胞(CT011)治疗,每个周期分为两次输注。在每次 CT011 治疗前,进行淋巴细胞耗竭。淋巴细胞耗竭方案为环磷酰胺 500mg/m/天,连用 2-3 天,氟达拉滨 20-25mg/m/天,连用 3-4 天。共输注 4×10 的 CAR-GPC3 T 细胞。CT011 联合索拉非尼治疗耐受性良好。所有≥3 级的 AEs 均为血液学毒性,被认为是预处理方案引起的预期事件。该患者在接受 CT011 输注后的第 3 个月达到部分缓解,并在第 1 个周期输注后 12 个月达到 CR,根据 RECIST1.1 评估。肿瘤 36 个月以上无进展,首次输注后 24 个月以上保持 CR 状态。