Lu Changchang, Zhu Yahui, Kong Weiwei, Yang Ju, Zhu Linxi, Wang Lei, Tang Min, Chen Jun, Li Qi, He Jian, Li Aimei, Qiu Xin, Gu Qing, Chen Dongsheng, Meng Fanyan, Liu Baorui, Qiu Yudong, Du Juan
The Comprehensive Cancer Center of Drum Tower Hospital, Medical School of Nanjing University, Nanjing, China.
Nanjing Drum Tower Hospital Clinical College of Nanjing University of Chinese Medicine, Nanjing, China.
Front Oncol. 2022 Aug 18;12:879661. doi: 10.3389/fonc.2022.879661. eCollection 2022.
Pancreatic ductal adenocarcinoma (PDAC) is a fatal malignancy with a low resection rate. Chemotherapy and radiotherapy (RT) are the main treatment approaches for patients with advanced pancreatic cancer, and neoadjuvant chemoradiotherapy is considered a promising strategy to increase the resection rate. Recently, immune checkpoint inhibitor (ICI) therapy has shown remarkable efficacy in several cancers. Therefore, the combination of ICI, chemotherapy, and concurrent radiotherapy is promising for patients with potentially resectable pancreatic cancer, mainly referring to locally advanced (LAPC) and borderline resectable pancreatic cancer (BRPC), to increase the chances of conversion to surgical resectability and prolong survival. This study aims to introduce the design of a clinical trial.
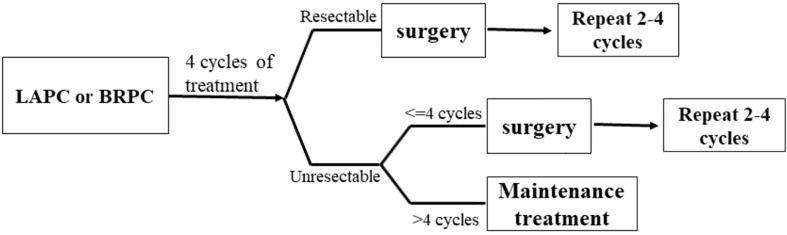
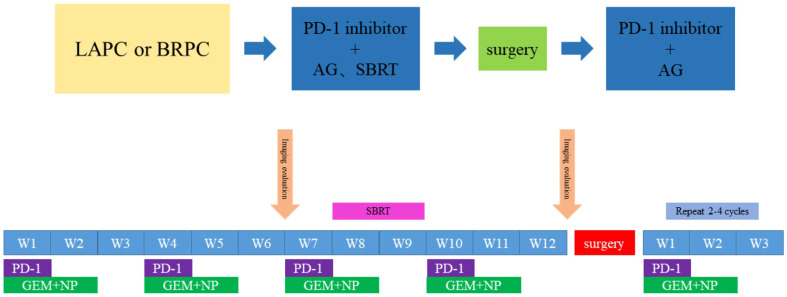
This is an open-label, single-arm, and single-center phase II trial. Patients with pathologically and radiographically confirmed LAPC or BRPC without prior anti-cancer treatment or severe morbidities will be enrolled. All patients will receive induction therapy and will be further evaluated by the Multiple Disciplinary Team (MDT) for the possibility of surgery. The induction therapy consists of up to four cycles of gemcitabine 1,000 mg/m and nab-paclitaxel 125 mg/m intravenous (IV) infusion on days 1 and 8, along with tislelizumab (a PD-1 monoclonal antibody) 200 mg administered through IV infusion on day 1 every 3 weeks, concurrently with stereotactic body radiation therapy (SBRT) during the third cycle of treatment. After surgery, patients without progression will receive another two to four cycles of adjuvant therapy with gemcitabine, nab-paclitaxel, and tislelizumab. The primary objectives are objective response rate (ORR) and the R0 resection rate. The secondary objectives are median overall survival (mOS), median progression free survival (mPFS), disease control rate (DCR), pathological grade of tumor tissue after therapy, and adverse reactions. Besides, we expect to explore the value of circulating tumor DNA (ctDNA) in predicting tumor response to induction therapy and survival outcome of patients.
This is a protocol for a clinical trial that attempts to evaluate the safety and efficacy of the combination of anti-PD-1 antibody plus chemotherapy and radiotherapy as the induction therapy for LAPC and BRPC. The results of this phase II study will provide evidence for the clinical practice of this modality.
http://www.chictr.org.cn/edit.aspx?pid=53720&htm=4, identifier ChiCTR2000032955.
胰腺导管腺癌(PDAC)是一种致命的恶性肿瘤,切除率较低。化疗和放疗(RT)是晚期胰腺癌患者的主要治疗方法,新辅助放化疗被认为是提高切除率的一种有前景的策略。最近,免疫检查点抑制剂(ICI)疗法在几种癌症中显示出显著疗效。因此,ICI、化疗和同步放疗联合应用对于潜在可切除的胰腺癌患者,主要是局部晚期(LAPC)和边界可切除胰腺癌(BRPC)患者,有望增加转化为手术可切除性的机会并延长生存期。本研究旨在介绍一项临床试验的设计。
这是一项开放标签、单臂、单中心的II期试验。将纳入经病理和影像学证实为LAPC或BRPC且未接受过先前抗癌治疗或无严重疾病的患者。所有患者将接受诱导治疗,并由多学科团队(MDT)进一步评估手术可能性。诱导治疗包括在第1天和第8天静脉输注(IV)吉西他滨1000mg/m²和白蛋白结合型紫杉醇125mg/m²,共四个周期,以及每3周在第1天静脉输注替雷利珠单抗(一种PD-1单克隆抗体)200mg,在治疗的第三个周期同时进行立体定向体部放疗(SBRT)。手术后,无进展的患者将接受另外两到四个周期的吉西他滨、白蛋白结合型紫杉醇和替雷利珠单抗辅助治疗。主要目标是客观缓解率(ORR)和R0切除率。次要目标是中位总生存期(mOS)、中位无进展生存期(mPFS)、疾病控制率(DCR)、治疗后肿瘤组织的病理分级以及不良反应。此外,我们期望探索循环肿瘤DNA(ctDNA)在预测肿瘤对诱导治疗的反应和患者生存结局方面的价值。
这是一项临床试验方案,旨在评估抗PD-1抗体联合化疗和放疗作为LAPC和BRPC诱导治疗的安全性和有效性。这项II期研究的结果将为这种治疗方式的临床实践提供证据。
http://www.chictr.org.cn/edit.aspx?pid=53720&htm=4,标识符ChiCTR2000032955。