De Placido Pietro, Pietroluongo Erica, De Angelis Carmine, Tafuro Margherita, Barraco Chiara, Giannatiempo Rosa, Buonaiuto Roberto, Schettini Francesco, Iervolino Anna, Vozzella Emilia Anna, Giuliano Mario, Bianco Roberto, Arpino Grazia
Department of Clinical Medicine and Surgery, University of Naples Federico II, Napoli, Campania, Italy.
Lester and Sue Smith Breast Center, Baylor College of Medicine, Houston, TX, United States.
Front Oncol. 2022 Aug 19;12:951026. doi: 10.3389/fonc.2022.951026. eCollection 2022.
Vaccines against severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) are highly effective. Nevertheless, immunocompromised participants were excluded from randomized controlled clinical trials. This study evaluates the efficacy and safety of the Pfizer/BioNTech BNT162b2 (BNT162b2) vaccine in patients with breast and gynecological cancer treated with active anticancer therapy versus a control cohort of healthy participants.
Immune responses to the BNT162b2 vaccine in patients with breast cancer ( = 44) or a gynecological malignancy ( = 6) on active anticancer therapy (28 on chemotherapy, mostly anthracycline- or taxane-based, and 22 on target therapy) and in a control cohort of participants without cancer ( = 67) were investigated by SARS-CoV-2 neutralizing antibody titers measured by S1-binding immunoglobulin G (IgG) concentrations assessed using the LIAISON XL tools (DiaSorin S.p.A.). Response was assessed after a second dose of the BNT162b2 vaccine administered before and at least 3 weeks after the vaccine dose.
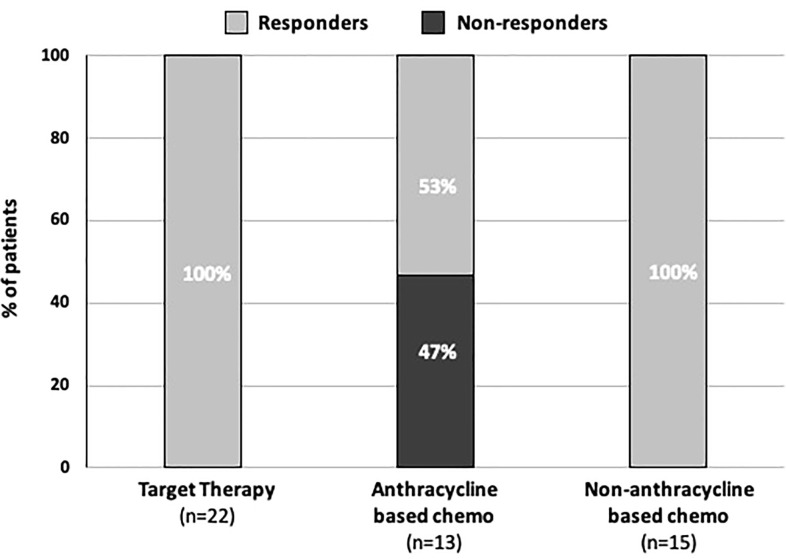
Overall, 43/50 (86%) patients of the cancer cohort (74% in the breast cancer group and 100% in the gynecological malignancy group) developed IgG antibodies after the second dose of the BNT162b2 vaccine. There were no statistically significant differences in responder rates between patients treated with chemotherapy and those on target therapy. The majority of patients who received chemotherapy with or without target therapy, 21/28 (75%), developed a reliable antibody titer after a vaccine. All seven non-responder patients were undergoing an anthracycline-based regimen. Based on IgG levels (0-400 AU/ml), patients were classified as negative ('non-responders'), weakly positive, or strongly positive ('responders'). No delay in cancer therapy schedule or reported side effects were recorded after BNT162b2 vaccine administration. All healthy participants were strongly positive. Responder rates differed significantly between the two study cohorts (p < 0.001).
Most patients develop antibody titers after the second immunization. However, given the persistence of non-responders or weak responders, additional immunization booster seems to be required, along with proactive planning in the vaccination schedule, with vaccine administration spaced out over time with respect to chemotherapy.
严重急性呼吸综合征冠状病毒2(SARS-CoV-2)疫苗非常有效。然而,免疫功能低下的参与者被排除在随机对照临床试验之外。本研究评估了辉瑞/ BioNTech BNT162b2(BNT162b2)疫苗在接受积极抗癌治疗的乳腺癌和妇科癌症患者与健康参与者对照队列中的疗效和安全性。
通过使用LIAISON XL工具(DiaSorin S.p.A.)评估的S1结合免疫球蛋白G(IgG)浓度测量的SARS-CoV-2中和抗体滴度,研究了接受积极抗癌治疗(28例接受化疗,主要基于蒽环类或紫杉烷类,22例接受靶向治疗)的乳腺癌患者(n = 44)或妇科恶性肿瘤患者(n = 6)以及无癌症参与者对照队列(n = 67)中对BNT162b2疫苗的免疫反应。在接种第二剂BNT162b2疫苗之前和接种疫苗后至少3周评估反应。
总体而言,癌症队列中的43/50(86%)患者(乳腺癌组为74%,妇科恶性肿瘤组为100%)在接种第二剂BNT162b2疫苗后产生了IgG抗体。接受化疗的患者与接受靶向治疗的患者之间的反应率没有统计学上的显著差异。大多数接受化疗(无论是否接受靶向治疗)的患者,21/28(75%),在接种疫苗后产生了可靠的抗体滴度。所有七名无反应患者均在接受基于蒽环类的方案。根据IgG水平(0 - 400 AU/ml),患者被分类为阴性(“无反应者”)、弱阳性或强阳性(“反应者”)。接种BNT162b2疫苗后未记录癌症治疗计划的延迟或报告的副作用。所有健康参与者均为强阳性。两个研究队列之间的反应率差异显著(p < 0.001)。
大多数患者在第二次免疫后产生抗体滴度。然而,鉴于无反应者或弱反应者的持续存在,似乎需要额外的免疫加强剂,同时在疫苗接种计划中进行积极规划,疫苗接种时间相对于化疗要间隔开。