Division of Cardiovascular Medicine, Department of Internal Medicine, University of Texas Southwestern Medical Center, Dallas (S.G.).
Saint Luke's Mid-America Heart Institute, Kansas City, MO (P.J).
Circ Cardiovasc Qual Outcomes. 2022 Sep;15(9):e008901. doi: 10.1161/CIRCOUTCOMES.122.008901. Epub 2022 Sep 6.
Although rapid response teams have been widely promoted as a strategy to reduce unexpected hospital deaths, most studies of rapid response teams have not adjusted for secular trends in mortality before their implementation. We examined whether implementation of a rapid response team was associated with a reduction in hospital mortality after accounting for preimplementation mortality trends.
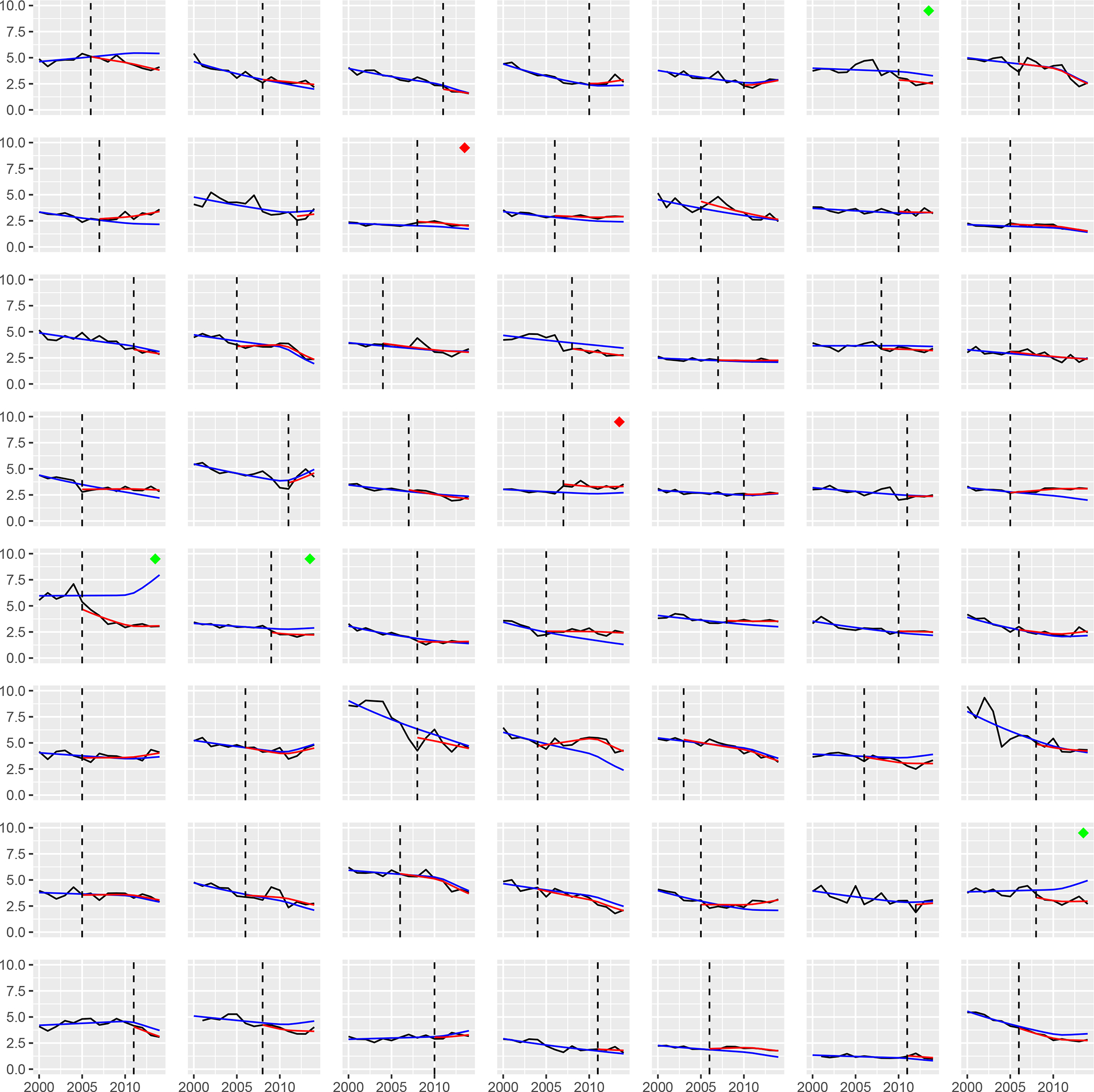
Among 56 hospitals in Get With The Guidelines-Resuscitation linked to Medicare, we calculated the annual rates of case mix-adjusted mortality for each hospital during 2000 to 2014. We constructed a hierarchical log-binomial regression model of mortality over time (calendar-year), incorporating terms to capture the effect of rapid response teams, to determine whether implementation of rapid response teams was associated with reduction in hospital mortality that was larger than expected based on preimplementation trends, while adjusting for hospital case mix index.
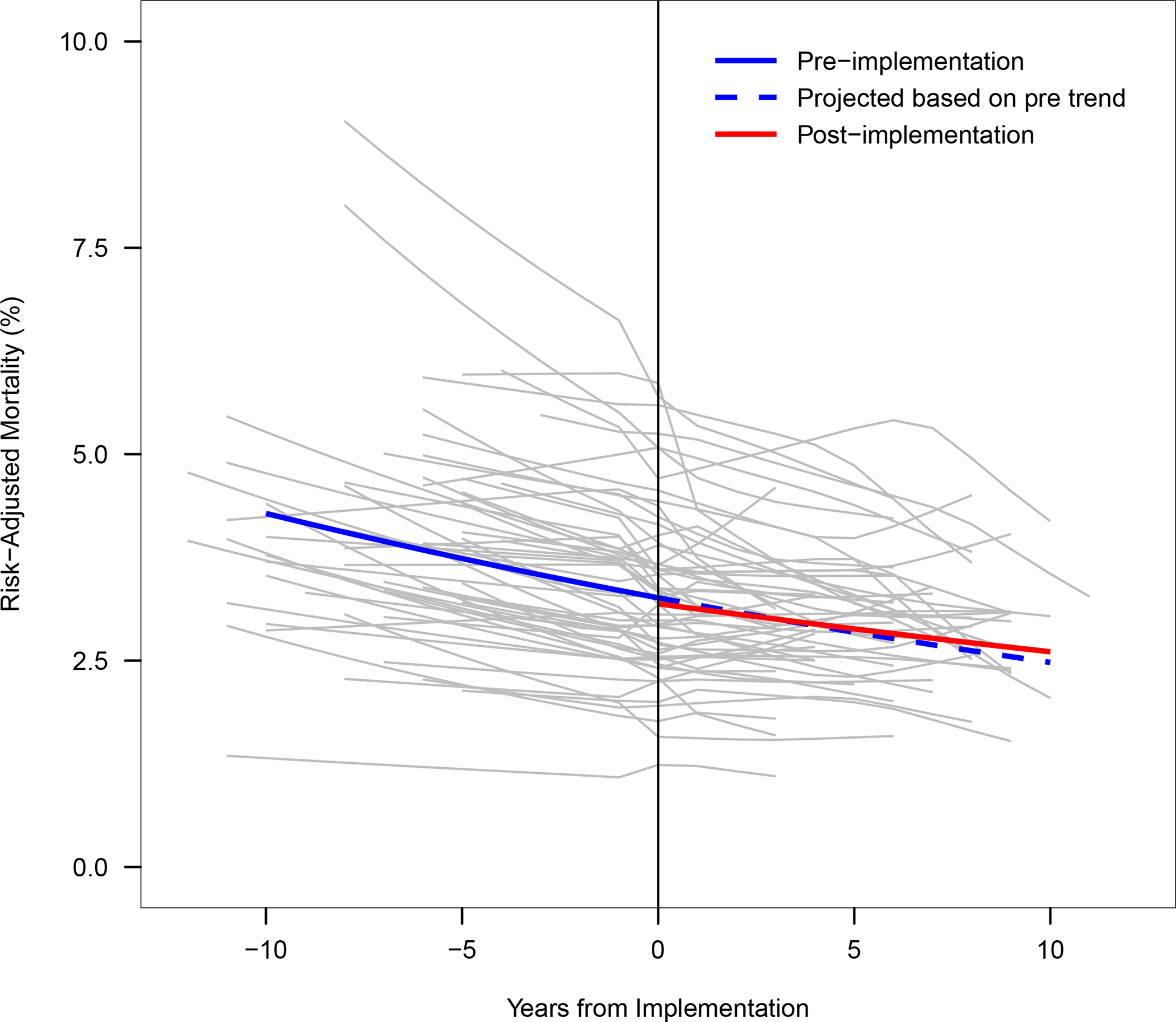
The median annual number of Medicare admissions was 5214 (range, 408-18 398). The median duration of preimplementation and postimplementation period was 7.6 years (≈2.5 million admissions) and 7.2 years (≈2.6 million admissions), respectively. Hospital mortality was decreasing by 2.7% annually during the preimplementation period. Implementation of rapid response teams was not associated with a change in mortality during the initial year (relative risk for model intercept, 0.98 [95% CI, 0.94-1.02]; =0.30) or in the mortality trend (relative risk for model slope, 1.01 per year [95% CI, 0.99-1.02]; =0.30). Among individual hospitals, implementation of a rapid response team was associated with a lower-than-expected mortality at only 4 (7.1%) and higher-than-expected mortality at 2 (3.7%) hospitals.
Among a large and diverse sample of US hospitals, we did not find implementation of rapid response teams to be associated with reduction in hospital mortality. Studies are needed to understand best practices for rapid response team implementation, to ensure that hospital investment in these teams improves patient outcomes.
尽管快速反应团队已被广泛推广作为降低医院意外死亡的策略,但大多数关于快速反应团队的研究在实施前都没有对死亡率的长期趋势进行调整。我们研究了在考虑实施前死亡率趋势的情况下,快速反应团队的实施是否与降低医院死亡率有关。
在与医疗保险相关的 Get With The Guidelines-Resuscitation 中,我们对 56 家医院进行了分析,计算了 2000 年至 2014 年期间每家医院的病例组合调整死亡率的年度比率。我们构建了一个时间(日历年度)死亡率的分层二项式回归模型,纳入了快速反应团队的效果项,以确定快速反应团队的实施是否与基于实施前趋势的医院死亡率降低有关,同时调整了医院病例组合指数。
医疗保险入院人数中位数为每年 5214 人(范围为 408-18398 人)。实施前和实施后时期的中位数持续时间分别为 7.6 年(约 250 万次入院)和 7.2 年(约 260 万次入院)。在实施前期间,医院死亡率每年下降 2.7%。在初始年份,快速反应团队的实施与死亡率的变化无关(模型截距的相对风险,0.98 [95% CI,0.94-1.02];=0.30),也与死亡率趋势无关(每年 1.01 的相对风险[95% CI,0.99-1.02];=0.30)。在个别医院中,只有 4 家(7.1%)医院的快速反应团队实施后死亡率低于预期,2 家(3.7%)医院的死亡率高于预期。
在一个大型且多样化的美国医院样本中,我们没有发现快速反应团队的实施与降低医院死亡率有关。需要进行研究以了解快速反应团队实施的最佳实践,以确保医院对这些团队的投资能够改善患者的预后。