Qi Litong, Chen Jiyan, Li Xiaodong, Qi Xiaoyong, Ding Chunhua, Chen Xiaoping, Gu Xiang, Xiao Wenliang, Zhao Shuiping, Dong Yugang, Zheng Mingqi, Huang Kai, Tang Liangqiu, Guo Xiaomei, Wang Fang, Fu Guosheng, Li Junxia, Huo Yong
Department of Cardiology, The First Hospital of Peking University, Beijing, China.
Department of Cardiology, Guangdong Provincial People's Hospital, Guangdong Academy of Medical Sciences, Guangzhou, China.
Front Cardiovasc Med. 2022 Aug 16;9:888604. doi: 10.3389/fcvm.2022.888604. eCollection 2022.
To evaluate the safety and efficacy of hybutimibe plus atorvastatin for lipid control in hypercholesterolemia patients with atherosclerotic cardiovascular disease risk equivalent.
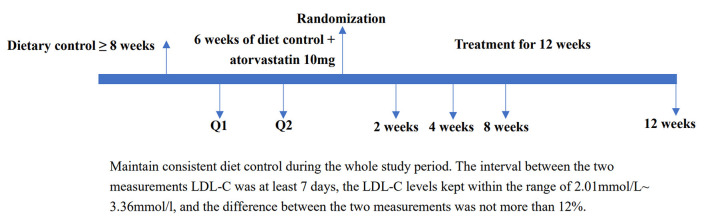
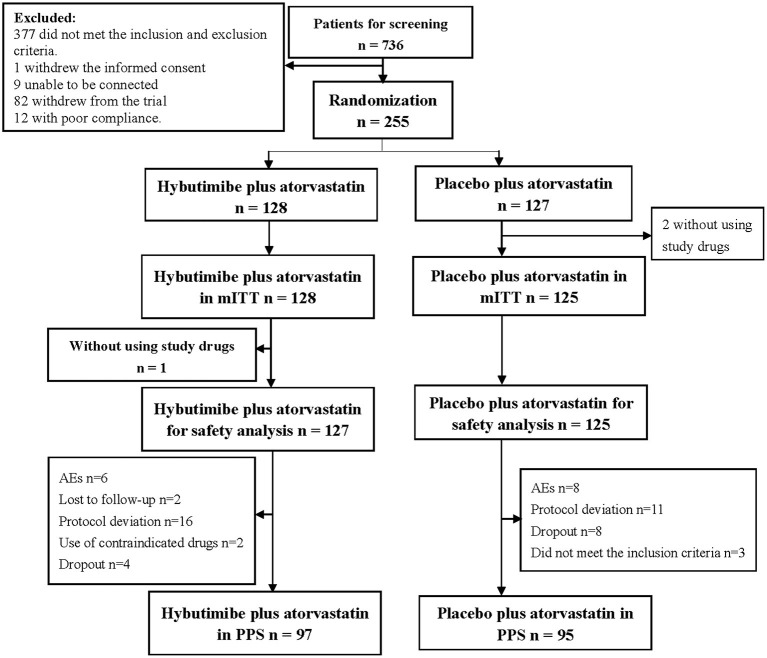
In this double-blind phase III study, we 1:1 randomly assigned 255 hypercholesterolemia patients with atherosclerotic cardiovascular disease to receive hybutimibe plus atorvastatin or placebo plus atorvastatin. The primary endpoint was the rate of change of plasma low-density lipoprotein-cholesterol (LDL-C) level at 12 weeks from baseline. The secondary endpoints were plasma total cholesterol (TC), triglyceride (TG), high-density lipoprotein-cholesterol (HDL-C), non-HDL-C, apoprotein (Apo) B, and 2-, 4-, 8-, and 12-week Apo A1 levels change rate and rates of change of plasma LDL-C levels at 2, 4, and 8 weeks from baseline.
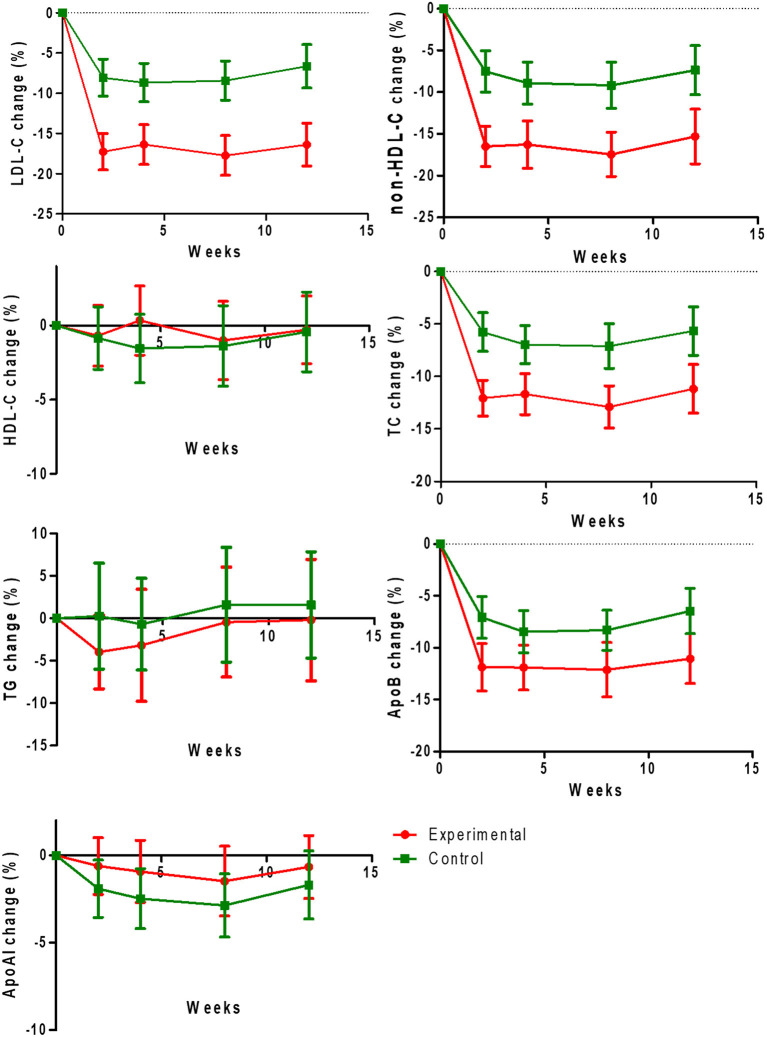
From April 2016 to January 2018, 128 in the hybutimibe plus atorvastatin group and 125 in the atorvastatin group were included in modified intention-to-treat (mITT) analysis. After 12 weeks of treatment, LDL-C level changed from 2.61 mmol/L (±0.30) at baseline to 2.18 mmol/L (±0.45) in the hybutimibe plus atorvastatin group and from 2.58 (±0.31) mmol/L to 2.40 (± 0.46) mmol/L in the atorvastatin group ( < 0.0001), in mITT. The change rate in the hybutimibe plus atorvastatin group was significantly higher than that in the atorvastatin group ( < 0.0001); the estimated mean rates of change were -16.39 (95% confidence interval: -19.04, -13.74) and -6.75 (-9.48, -4.02), respectively. Consistently, in per-protocol set (PPS) analysis, the rate of change of LDL-C in the hybutimibe plus atorvastatin group was significantly higher than that in atorvastatin group. Significant decreases in the change rates of non-HDL-C, TC, and Apo B at 2, 4, 8, and 12 weeks (all < 0.05) were observed for hybutimibe plus atorvastatin, while the differences were not significant for HDL-C, TG, and Apo-A1 (all > 0.05). During the study period, no additional side effects were reported.
Hybutimibe combined with atorvastatin resulted in significant improvements in LDL-C, non-HDL-C, TC, and Apo B compared with atorvastatin alone. The safety and tolerability were also acceptable, although additional benefits of hybutimibe plus atorvastatin were not observed compared with atorvastatin alone in HDL-C, TG, and Apo-A1.
评估海布替米贝联合阿托伐他汀对具有动脉粥样硬化性心血管疾病风险等同的高胆固醇血症患者血脂控制的安全性和有效性。
在这项双盲III期研究中,我们将255例患有动脉粥样硬化性心血管疾病的高胆固醇血症患者按1:1随机分配,分别接受海布替米贝联合阿托伐他汀或安慰剂联合阿托伐他汀治疗。主要终点是12周时血浆低密度脂蛋白胆固醇(LDL-C)水平相对于基线的变化率。次要终点是血浆总胆固醇(TC)、甘油三酯(TG)、高密度脂蛋白胆固醇(HDL-C)、非HDL-C、载脂蛋白(Apo)B以及2周、4周、8周和12周时Apo A1水平的变化率,以及血浆LDL-C水平相对于基线在2周、4周和8周时的变化率。
从2016年4月至2018年1月,海布替米贝联合阿托伐他汀组128例和阿托伐他汀组125例纳入改良意向性分析(mITT)。治疗12周后,在mITT中,海布替米贝联合阿托伐他汀组LDL-C水平从基线时的2.61 mmol/L(±0.30)降至2.18 mmol/L(±0.45),阿托伐他汀组从2.58(±0.31)mmol/L降至2.40(±0.46)mmol/L(P<0.0001)。海布替米贝联合阿托伐他汀组的变化率显著高于阿托伐他汀组(P<0.0001);估计平均变化率分别为-16.39(95%置信区间:-19.04,-13.74)和-6.75(-9.48,-4.02)。同样,在符合方案集(PPS)分析中,海布替米贝联合阿托伐他汀组LDL-C的变化率显著高于阿托伐他汀组。观察到海布替米贝联合阿托伐他汀在2周、4周、8周和12周时非HDL-C、TC和Apo B的变化率显著降低(均P<0.05),而HDL-C、TG和Apo-A1的差异不显著(均P>0.05)。在研究期间,未报告额外的副作用。
与单独使用阿托伐他汀相比,海布替米贝联合阿托伐他汀可显著改善LDL-C、非HDL-C、TC和Apo B。安全性和耐受性也可接受,尽管在HDL-C、TG和Apo-A1方面,与单独使用阿托伐他汀相比,未观察到海布替米贝联合阿托伐他汀有额外益处。