Lanzhou University, Lanzhou, 730000, Gansu, China.
Department of Cardiology, Gansu Provincial People's Hospital, Lanzhou, 730000, Gansu, China.
BMC Cardiovasc Disord. 2022 Sep 8;22(1):402. doi: 10.1186/s12872-022-02834-z.
The precise clinical features and etiologic basis of Takotsubo syndrome remain unclear, although an association with emotional or stressful triggers has been recognized. Ventricular septal perforation is a very rare life-threatening complication.
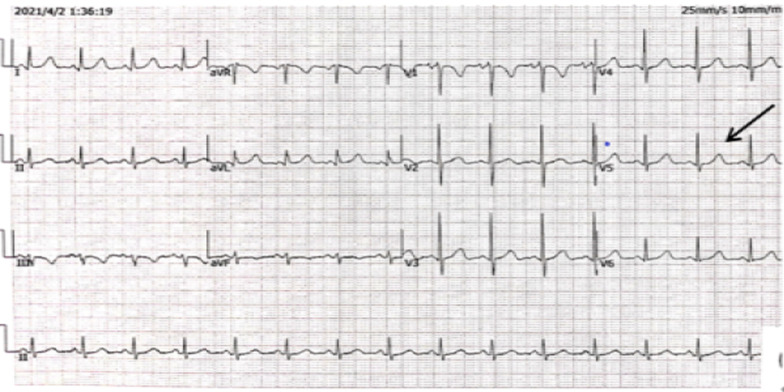
A 77-year-old female patient presented to the hospital with unrelieved chest tightness and shortness of breath. Three months ago, the patient's electrocardiogram revealed ischemic T wave inversion of the anterior wall, along with an increase in myocardial injury markers. There was no evidence of a ventricular septal defect on echocardiography. The patient was admitted to the respiratory department to treat lung lesions. The electrocardiogram demonstrated dynamic changes following admission, and the myocardial markers returned to normal, but the echocardiography revealed a ventricular septal defect. The initial diagnosis was ventricular septal perforation because of myocardial infarction with acute anterior ST-segment elevation. Coronary angiography revealed no abnormalities, but left ventricular angiography revealed an enlarged apex and VSD, with a right ventricular shunt bundle. Later, cardiac MRI revealed an apical ventricular septal defect. Further inquiry of the patient's medical history revealed that her husband died unexpectedly three months ago, and her daughter was seriously injured in a car accident, causing the patient severe emotional distress. Takotsubo syndrome was then determined in conjunction with the patient's medical history, symptoms, signs, and pertinent examinations. Without using a catheter or a surgical procedure, we managed the patient's medical condition. Two weeks later, the patient was discharged with symptoms improved.
Takotsubo syndrome is comparable to an acute myocardial infarction on clinical and electrocardiographic examination in the absence of significant coronary disease. Although ventricular septal perforation is most commonly associated with acute myocardial infarction, it can also happen following Takotsubo syndrome. Takotsubo syndrome complicated by ventricular septal perforation is easily misdiagnosed. The early recognition and management of this condition can avoid or reduce morbidity and mortality.
尽管已经认识到 Takotsubo 综合征与情绪或应激性触发因素有关,但该疾病的确切临床特征和病因基础仍不清楚。室间隔穿孔是一种非常罕见的危及生命的并发症。
一名 77 岁女性患者因持续的胸闷和呼吸急促到医院就诊。三个月前,患者的心电图显示前壁缺血性 T 波倒置,同时心肌损伤标志物升高。超声心动图未见室间隔缺损。患者因肺部病变入住呼吸科。入院后心电图显示动态变化,心肌标志物恢复正常,但超声心动图显示室间隔缺损。最初的诊断是由于急性前壁 ST 段抬高型心肌梗死导致的室间隔穿孔。冠状动脉造影未见异常,但左心室造影显示心尖部扩大和 VSD,并伴有右心室束分流。后来,心脏 MRI 显示心尖部室间隔缺损。进一步询问患者病史发现,她的丈夫三个月前意外去世,女儿在车祸中受重伤,这让患者情绪极度痛苦。结合患者的病史、症状、体征和相关检查,诊断为 Takotsubo 综合征。我们没有使用导管或手术来治疗患者的病情。两周后,患者症状改善出院。
Takotsubo 综合征在无明显冠状动脉疾病的情况下,在临床和心电图检查上与急性心肌梗死相似。尽管室间隔穿孔最常与急性心肌梗死有关,但也可发生于 Takotsubo 综合征之后。Takotsubo 综合征并发室间隔穿孔容易误诊。早期识别和处理这种情况可以避免或减少发病率和死亡率。