Wang Yong, Guo Wei, Ma Jianliang
Department of Cardiology, Affiliated Hospital of Shandong University of Traditional Chinese Medicine.
Department of Cardiology, Shuguang Hospital Affiliated to Shanghai University of Traditional Chinese Medicine, China.
Medicine (Baltimore). 2019 Mar;98(9):e14677. doi: 10.1097/MD.0000000000014677.
The clinical features of Takotsubo cardiomyopathy largely overlap with those of acute myocardial infarction, especially in the presence of ST-segment elevation on the initial electrocardiogram. Giant R wave syndrome has mainly been observed in the hyperacute phase of acute myocardial infarction.
In this study, we report a unique case of Takotsubo cardiomyopathy that caused giant R wave syndrome.
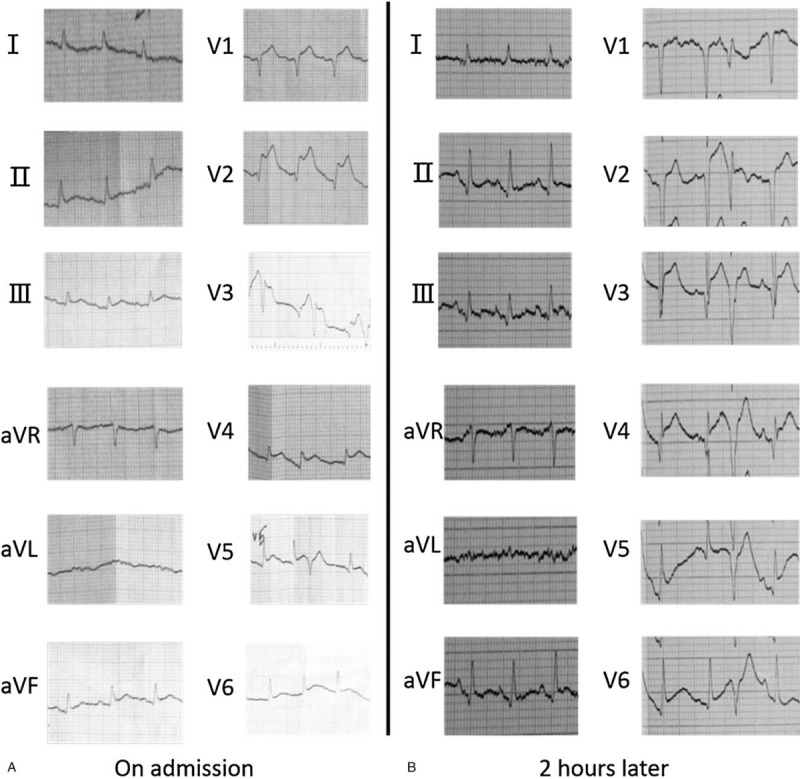
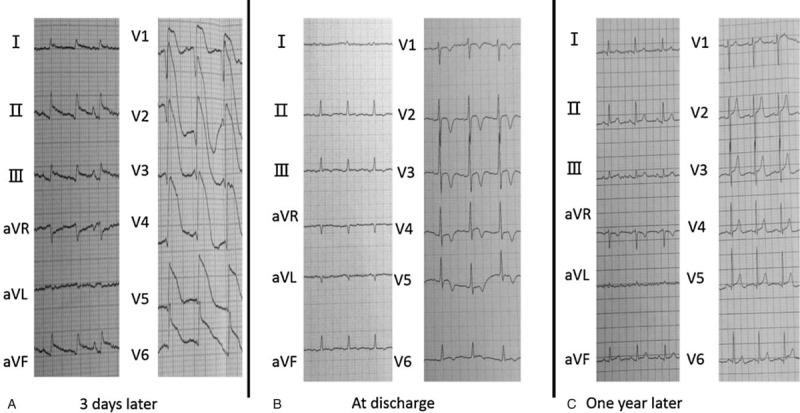
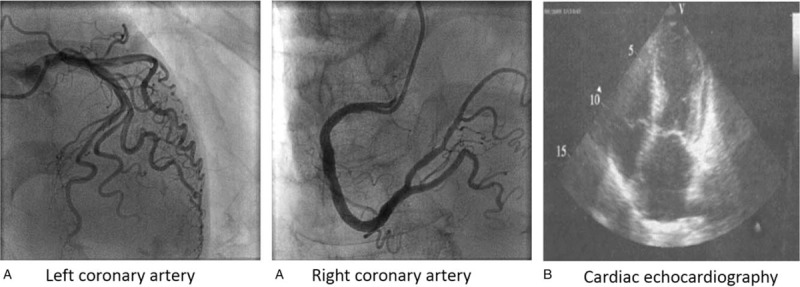
A 71-year-old woman was transferred to hospital with new onset chest pain. An initial electrocardiogram showed ST-segment elevation in the inferior wall and anterior wall leads. Her initial cardiac troponin I levels were elevated. Acute myocardial infarction was suspected and the patient underwent emergent cardiac catheterization. A coronary angiography showed no overt stenosis in the coronary artery. After 2 hours, her chest pain disappeared and an electrocardiogram revealed that the ST segment had decreased markedly. However, on day 3, an electrocardiogram of the V1-V6 leads revealed the formation of giant R wave syndrome: giant R waves merging with the markedly elevated ST segments and the obliteration of S waves. Cardiac echocardiography showed hypokinetic apical mid-segments and hyperkinetic basal segments of the left ventricle, low left ventricular ejection (42%), and enlargement of the left ventricle. On the basis of these findings, the patient was diagnosed with early recurrent Takotsubo cardiomyopathy.
The patient has been treated by levosimendan and furosemide to improve cardiac function before leaving the hospital. After discharge, she was treated with a beta blocker.
The patient was discharged 2 weeks later in stable condition without chest pain. One year later, during her follow-up, a repeat echocardiogram and ECG showed normal findings.
To the best of our knowledge, this is the first report of giant R wave syndrome on electrocardiogram following Takotsubo cardiomyopathy. Takotsubo cardiomyopathy, especially presenting with giant R wave syndrome on electrocardiogram, remains a challenging condition given its similarity to acute myocardial infarction in its early phase.
应激性心肌病的临床特征与急性心肌梗死的临床特征在很大程度上重叠,尤其是在初始心电图出现ST段抬高时。巨大R波综合征主要在急性心肌梗死的超急性期观察到。
在本研究中,我们报告了1例导致巨大R波综合征的独特应激性心肌病病例。
一名71岁女性因新发胸痛被转诊至医院。初始心电图显示下壁和前壁导联ST段抬高。其初始心肌肌钙蛋白I水平升高。怀疑为急性心肌梗死,患者接受了紧急心脏导管插入术。冠状动脉造影显示冠状动脉无明显狭窄。2小时后,她的胸痛消失,心电图显示ST段明显下降。然而,在第3天,V1-V6导联的心电图显示巨大R波综合征形成:巨大R波与明显抬高的ST段融合,S波消失。心脏超声心动图显示左心室心尖中段运动减弱、基底段运动增强,左心室射血分数低(42%),左心室扩大。基于这些发现,该患者被诊断为早期复发性应激性心肌病。
患者在出院前接受了左西孟旦和呋塞米治疗以改善心功能。出院后,她接受了β受体阻滞剂治疗。
患者2周后出院,病情稳定,无胸痛。1年后随访时,重复超声心动图和心电图检查结果正常。
据我们所知,这是应激性心肌病后心电图出现巨大R波综合征的首例报告。应激性心肌病,尤其是心电图表现为巨大R波综合征时,因其在早期与急性心肌梗死相似,仍然是一种具有挑战性的病症。