Marcus Rebecca, Christopher Wade, Keller Jennifer, Nassoiy Sean, Chang Shu-Ching, Goldfarb Melanie, Wolf Ronald, Jutric Zeljka
Department of Surgical Oncology, Providence Saint John's Cancer Institute, Santa Monica, CA 90404, USA.
Medical Data Research Center, Providence Saint Joseph Health, Portland, OR 97229, USA.
Cancers (Basel). 2022 Sep 3;14(17):4320. doi: 10.3390/cancers14174320.
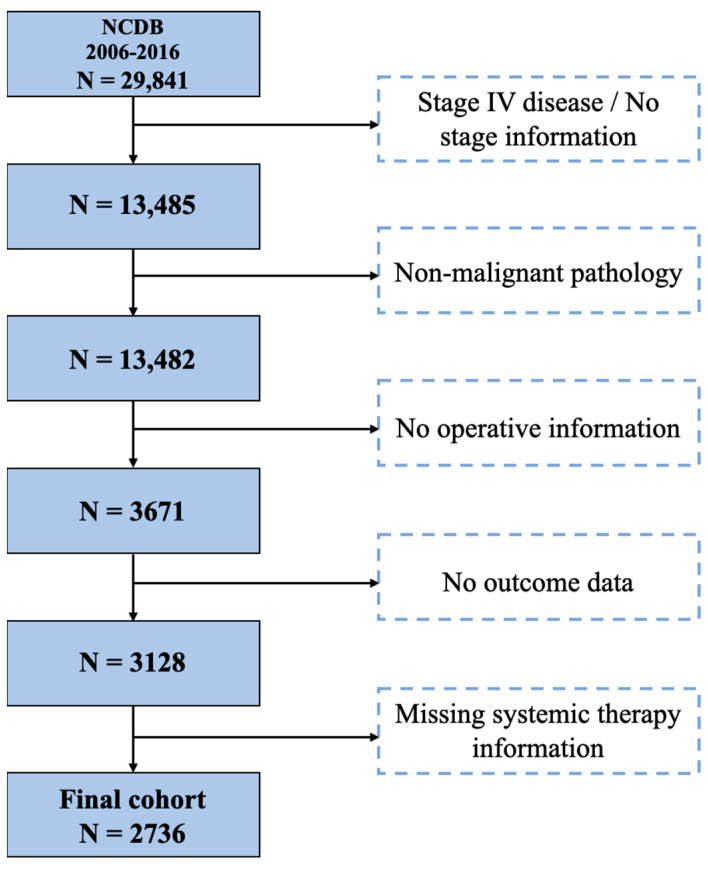
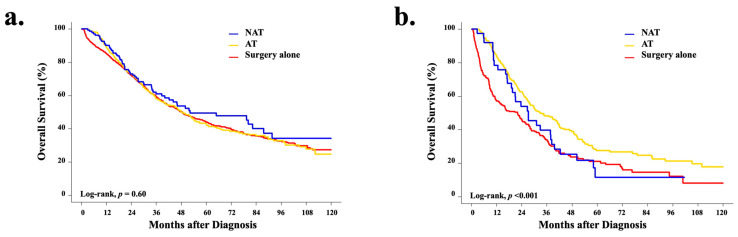
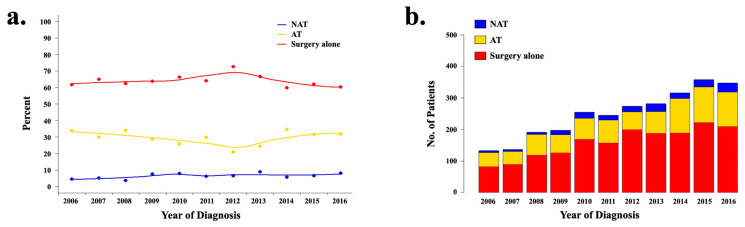
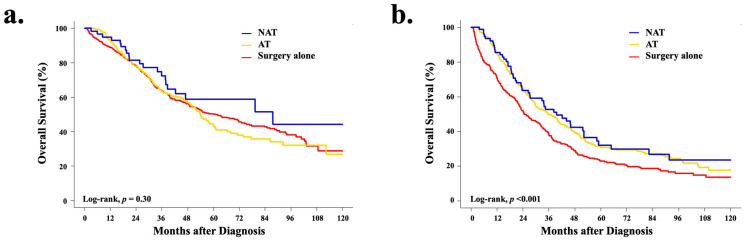
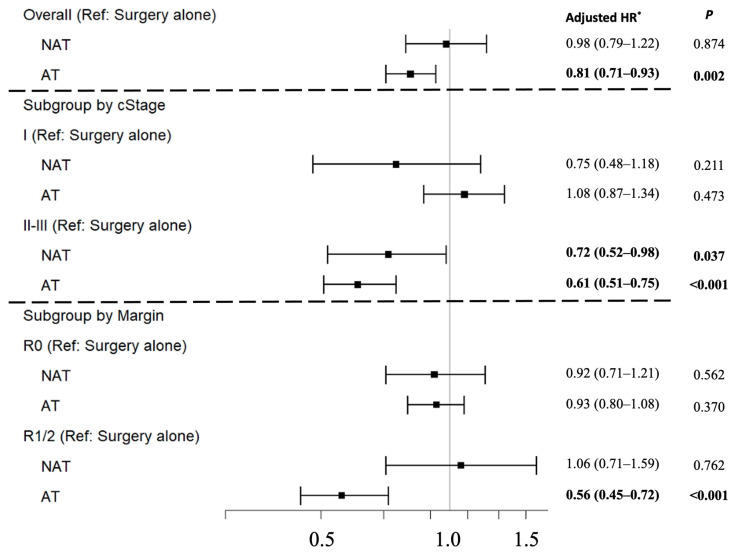
Limited evidence-based management guidelines for resectable intrahepatic cholangiocarcinoma (ICC) currently exist. Using a large population-based cancer registry; the utilization rates and outcomes for patients with clinical stages I-III ICC treated with neoadjuvant chemotherapy (NAT) in relation to other treatment strategies were investigated, as were the predictors of treatment regimen utilization. Oncologic outcomes were compared between treatment strategies. Amongst 2736 patients, chemotherapy utilization was low; however, NAT use increased from 4.3% to 7.2% ( = 0.011) over the study period. A higher clinical stage was predictive of the use of NAT, while higher pathologic stage and margin-positive resections were predictive of the use of adjuvant therapy (AT). For patients with more advanced disease, the receipt of NAT or AT was associated with significantly improved survival compared to surgery alone (cStage II, = 0.040; cStage III, = 0.003). Furthermore, patients receiving NAT were more likely to undergo margin-negative resections compared to those treated with AT (72.5% vs. 62.6%, = 0.027), despite having higher-risk tumors. This analysis of treatment strategies for resectable ICC suggests a benefit for systemic therapy. Prospective and randomized studies evaluating the sequencing of treatments for patients with high-risk resectable ICC are needed.
目前,关于可切除性肝内胆管癌(ICC)的循证管理指南有限。利用一个大型的基于人群的癌症登记处,研究了I - III期ICC患者接受新辅助化疗(NAT)与其他治疗策略相比的使用率和治疗结果,以及治疗方案使用的预测因素。比较了不同治疗策略之间的肿瘤学结果。在2736例患者中,化疗使用率较低;然而,在研究期间,NAT的使用从4.3%增加到7.2%(P = 0.011)。较高的临床分期可预测NAT的使用,而较高的病理分期和切缘阳性切除术可预测辅助治疗(AT)的使用。对于疾病进展较严重的患者,与单纯手术相比,接受NAT或AT与显著改善的生存率相关(cStage II,P = 0.040;cStage III,P = 0.003)。此外,与接受AT治疗的患者相比,接受NAT治疗的患者更有可能进行切缘阴性切除术(72.5%对62.6%,P = 0.027),尽管其肿瘤风险更高。这项对可切除性ICC治疗策略的分析表明全身治疗有益。需要开展前瞻性随机研究,以评估高危可切除性ICC患者的治疗顺序。