Institut of Biomedical Research August Pi i Sunyer (IDIBAPS), 08036 Barcelona, Spain.
Laboratory of Human Genome and Multifactorial Diseases (LR12ES07), Faculty of Pharmacy, University of Monastir, Monastir 5000, Tunisia.
Cells. 2022 Sep 5;11(17):2763. doi: 10.3390/cells11172763.
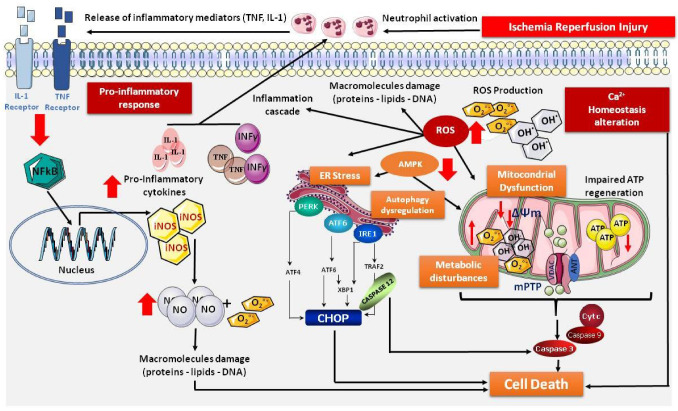
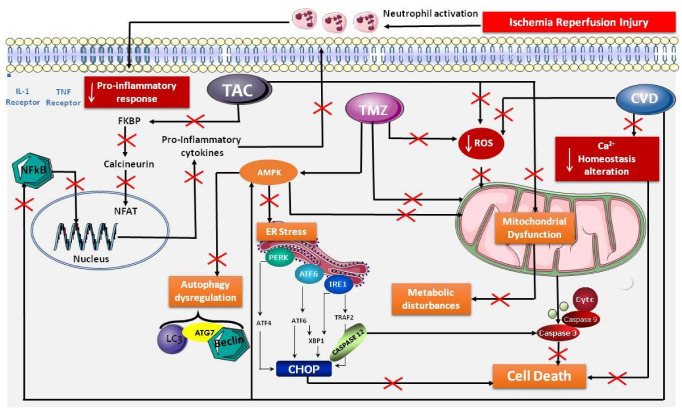
The pathophysiological process of ischemia and reperfusion injury (IRI), an inevitable step in organ transplantation, causes important biochemical and structural changes that can result in serious organ damage. IRI is relevant for early graft dysfunction and graft survival. Today, in a global context of organ shortages, most organs come from extended criteria donors (ECDs), which are more sensitive to IRI. The main objective of organ preservation solutions is to protect against IRI through the application of specific, nonphysiological components, under conditions of no blood or oxygen, and then under conditions of metabolic reduction by hypothermia. The composition of hypothermic solutions includes osmotic and oncotic buffering components, and they are intracellular (rich in potassium) or extracellular (rich in sodium). However, above all, they all contain the same type of components intended to protect against IRI, such as glutathione, adenosine and allopurinol. These components have not changed for more than 30 years, even though our knowledge of IRI, and much of the relevant literature, questions their stability or efficacy. In addition, several pharmacological molecules have been the subjects of preclinical studies to optimize this protection. Among them, trimetazidine, tacrolimus and carvedilol have shown the most benefits. In fact, these drugs are already in clinical use, and it is a question of repositioning them for this novel use, without additional risk. This new strategy of including them would allow us to shift from cold storage solutions to cold preservation solutions including multitarget pharmacological components, offering protection against IRI and thus protecting today's more vulnerable organs.
缺血再灌注损伤(IRI)的病理生理过程是器官移植中不可避免的一步,它会导致重要的生化和结构变化,从而导致严重的器官损伤。IRI 与早期移植物功能障碍和移植物存活有关。如今,在全球器官短缺的背景下,大多数器官都来自扩展标准供者(ECD),它们对 IRI 更为敏感。器官保存液的主要目的是通过应用特定的、非生理成分来防止 IRI,在没有血液或氧气的情况下,并在通过低温降低代谢的情况下。低温保存液的成分包括渗透和粘弹性缓冲成分,它们是细胞内(富含钾)或细胞外(富含钠)的。然而,最重要的是,它们都含有相同类型的成分,旨在防止 IRI,如谷胱甘肽、腺嘌呤和别嘌呤醇。这些成分 30 多年来没有变化,尽管我们对 IRI 的了解以及相关文献的大部分内容都对它们的稳定性或疗效提出了质疑。此外,几种药理分子已成为临床前研究的主题,以优化这种保护。其中,曲美他嗪、他克莫司和卡维地洛显示出最大的益处。事实上,这些药物已经在临床使用,问题是将它们重新定位用于这种新用途,而不会增加额外的风险。这种包含它们的新策略将使我们能够从冷藏溶液转变为包含多靶点药理成分的冷藏保存溶液,从而提供对 IRI 的保护,从而保护当今更脆弱的器官。