Miki Masami, Fujimori Nao, Ueda Keijiro, Lee Lingaku, Murakami Masatoshi, Takamatsu Yu, Shimokawa Yuzo, Niina Yusuke, Oono Takamasa, Hisano Terumasa, Furukawa Masayuki, Ogawa Yoshihiro
Department of Hepato-Biliary-Pancreatology, National Hospital Organization, Kyushu Cancer Center, Fukuoka 811-1347, Japan.
Department of Medicine and Bioregulatory Science, Graduate School of Medical Sciences, Kyushu University, Fukuoka 812-8582, Japan.
J Clin Med. 2022 Aug 30;11(17):5084. doi: 10.3390/jcm11175084.
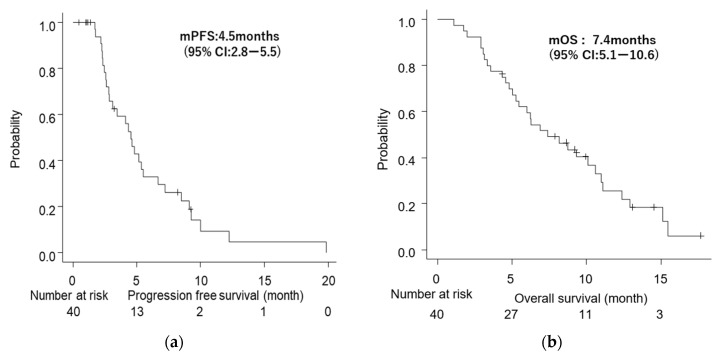
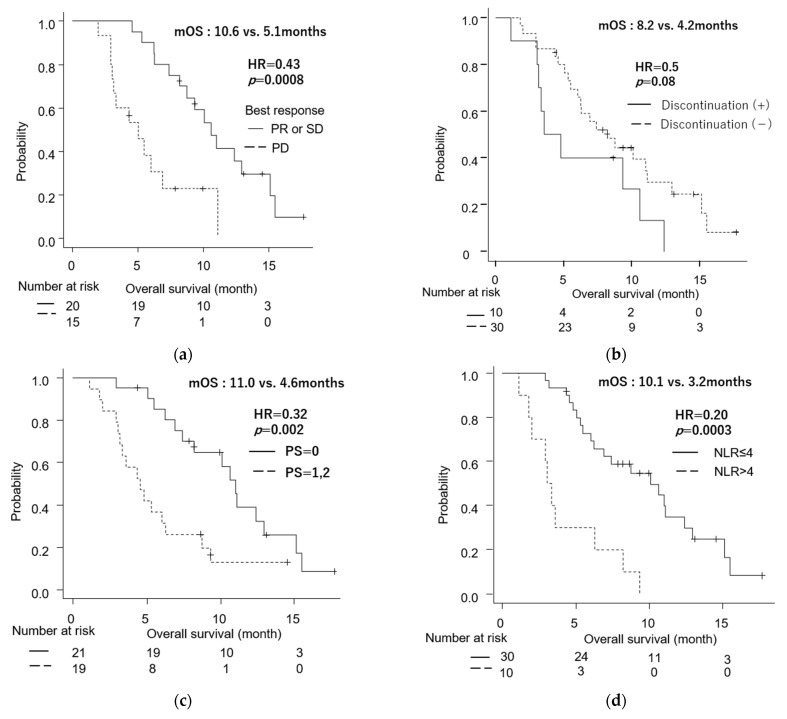
Although the combination of nanoliposomal irinotecan plus fluorouracil/folinic acid (nal-IRI/FF) exhibited survival benefits in gemcitabine-refractory patients with advanced pancreatic cancer (APC) in the phase III NAPOLI-1 trial, there is limited data on the efficacy and safety of this regimen in real-world settings in Japan. This multicenter, prospective observational study enrolled patients with APC who received nal-IRI/FF after a gemcitabine-based regimen from July 2020 to June 2021. We collected and analyzed clinical data and conducted survival and multivariate analyses. Thirty-one (78%) of the 40 patients had metastases. Nal-IRI/FF was the second-line therapy in 36 patients (90%). The median duration was 3.2 months. The disease control rate was 57%. The median progression-free survival and overall survival (OS) were 4.5 months (95% confidence interval [CI]: 2.8−5.5) and 7.4 months (95% CI: 5.1−10.6), respectively. Common ≥grade 3 toxicities included neutropenia (28%) and fatigue (23%). Fatigue led to treatment discontinuation in 6 out of 10 patients. Multivariate analysis showed that a neutrophil-to-lymphocyte ratio > 4 was a significant risk factor for a short OS (hazard ratio (HR) = 3.08, 95% CI: 1.21−7.85, p = 0.02). In conclusion, nal-IRI/FF is an appropriate treatment option for APC following gemcitabine-containing regimens.
尽管在III期NAPOLI-1试验中,纳米脂质体伊立替康联合氟尿嘧啶/亚叶酸(nal-IRI/FF)对吉西他滨难治的晚期胰腺癌(APC)患者显示出生存获益,但在日本真实世界环境中,关于该方案疗效和安全性的数据有限。这项多中心前瞻性观察性研究纳入了2020年7月至2021年6月期间接受基于吉西他滨方案治疗后再接受nal-IRI/FF治疗的APC患者。我们收集并分析了临床数据,并进行了生存和多因素分析。40例患者中有31例(78%)发生转移。nal-IRI/FF是36例患者(90%)的二线治疗方案。中位治疗持续时间为3.2个月。疾病控制率为57%。中位无进展生存期和总生存期(OS)分别为4.5个月(95%置信区间[CI]:2.8−5.5)和7.4个月(95%CI:5.1−10.6)。常见的≥3级毒性包括中性粒细胞减少(28%)和疲劳(23%)。10例患者中有6例因疲劳导致治疗中断。多因素分析显示,中性粒细胞与淋巴细胞比值>4是OS短的显著危险因素(风险比[HR]=3.08,95%CI:1.21−7.85,p=0.02)。总之,nal-IRI/FF是含吉西他滨方案治疗后APC的合适治疗选择。