Department of Medicine, Division of Hematology/Oncology, David Geffen School of Medicine, University of California Los Angeles, Los Angeles, CA, USA.
Notre Dame University, Fremantle and Edith Cowan University Joondalup, Perth, Australia.
BMC Cancer. 2020 Jul 8;20(1):633. doi: 10.1186/s12885-020-07110-x.
Pancreatic cancer has a poor prognosis and few choices of therapy. For patients with adequate performance status, FOLFIRINOX or gemcitabine plus nab-paclitaxel are preferred first-line treatment. 5-Fluorouracil (5-FU)-based therapy (e.g. FOLFIRI, OFF, or FOLFOX) are often used in patients who previously received gemcitabine-based regimens. A systematic review was conducted of the safety and efficacy of FOLFOX for metastatic pancreatic cancer following prior gemcitabine-based therapy. A Bayesian fixed-effect meta-analysis with adjustment of patient performance status (PS) was conducted to evaluate overall survival (OS) and compare outcomes with nanoliposomal irinotecan combination therapy.
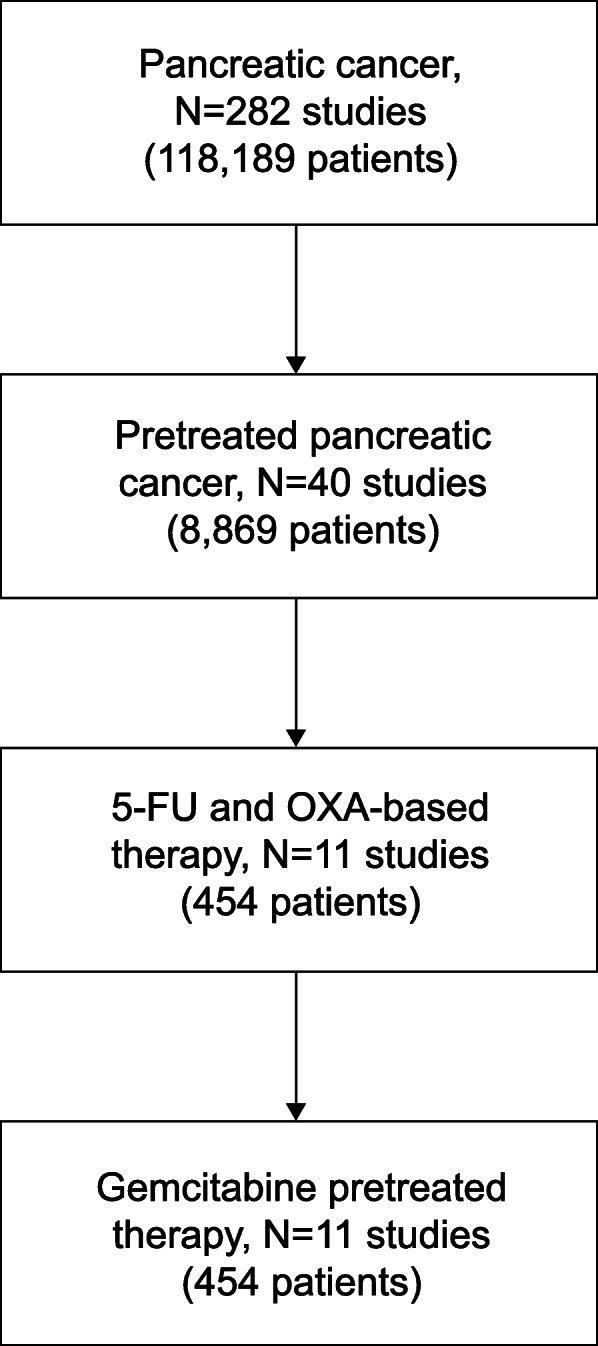
PubMed.gov , FDA.gov , ClinicalTrials.gov , congress abstracts, Cochrane.org library, and EMBASE database searches were conducted to identify randomized controlled trials of advanced/metastatic disease, prior gemcitabine-based therapy, and second-line treatment with 5-FU and oxaliplatin. The database search dates were January 1, 1990-June 30, 2019. Endpoints were OS and severe treatment-related adverse events (TRAEs). Trial-level PS scores were standardized by converting Karnofsky grade scores to Eastern Cooperative Oncology Group (ECOG) Grade, and overall study-weighted PS was calculated based on weighted average of all patients.
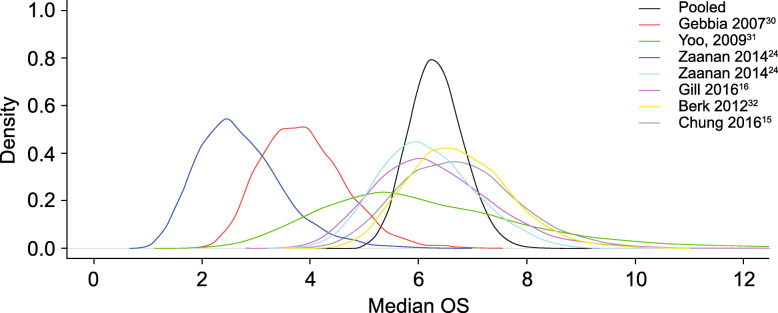
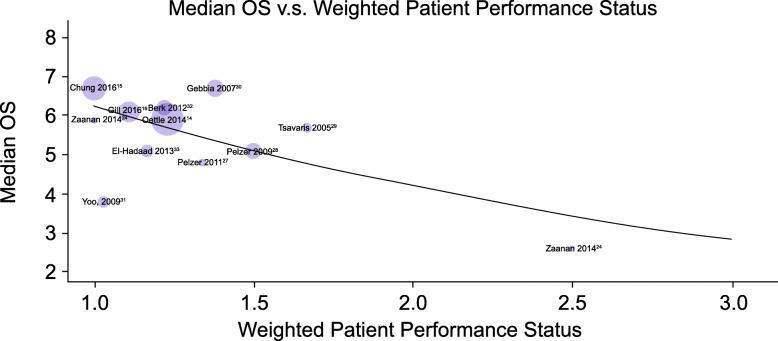
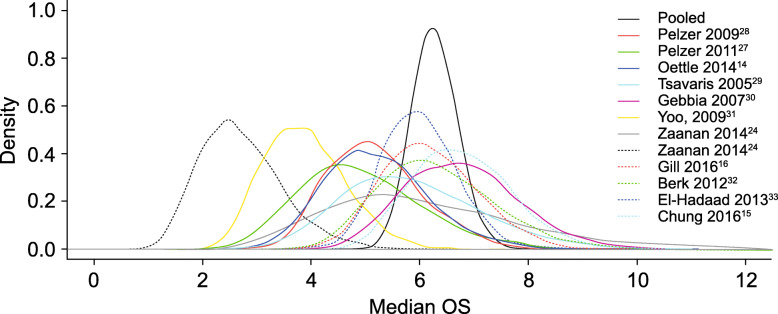
Of 282 studies identified, 11 randomized controlled trials (N = 454) were included in the meta-analysis. Baseline weighted PS scores predicted OS in 10 of the 11 studies, and calculated PS scores of 1.0 were associated with a median OS of 6.3 months (95% posterior interval, 5.4-7.4). After adjusting for baseline PS, FOLFOX had a similar treatment effect profile (median OS, range 2.6-6.7 months) as 5-FU/leucovorin plus nanoliposomal irinotecan therapy (median OS, 6.1 months; 95% confidence interval 4.8-8.9). Neutropenia and fatigue were the most commonly reported Grade 3-4 TRAEs associated with FOLFOX.
Baseline PS is a strong prognostic factor when interpreting the efficacy of 5-FU and oxaliplatin-based therapy of pancreatic cancer after progression on first-line gemcitabine-based regimens. When baseline PS is considered, FOLFOX has a similar treatment effect as 5-FU and nanoliposomal irinotecan therapy and a comparable safety profile. These findings suggest that 5-FU and oxaliplatin-based therapies remain an acceptable and alternative second-line treatment option for patients with pancreatic cancer and adequate PS (e.g. ECOG 0-1) following gemcitabine treatment.
胰腺癌预后较差,治疗选择有限。对于一般身体状况良好的患者,首选 FOLFIRINOX 或吉西他滨联合 nab-紫杉醇作为一线治疗。5-氟尿嘧啶(5-FU)为基础的治疗(如 FOLFIRI、OFF 或 FOLFOX)通常用于之前接受过吉西他滨为基础的治疗方案的患者。本文对先前接受过吉西他滨为基础的治疗方案的转移性胰腺癌患者进行了基于氟尿嘧啶(5-FU)和奥沙利铂的 FOLFOX 治疗的安全性和有效性的系统评价。采用贝叶斯固定效应荟萃分析,并调整患者的体能状态(PS),评估总生存期(OS)并与纳米脂质体伊立替康联合治疗进行比较。
对 PubMed.gov、FDA.gov、ClinicalTrials.gov、会议摘要、Cochrane.org 图书馆和 EMBASE 数据库进行了检索,以确定晚期/转移性疾病、先前接受过吉西他滨为基础的治疗以及二线治疗使用氟尿嘧啶和奥沙利铂的随机对照试验。数据库搜索日期为 1990 年 1 月 1 日至 2019 年 6 月 30 日。终点为 OS 和严重治疗相关不良事件(TRAEs)。试验级 PS 评分通过将卡氏评分转换为东部合作肿瘤学组(ECOG)评分进行标准化,并根据所有患者的加权平均值计算总体研究加权 PS。
在 282 项研究中,有 11 项随机对照试验(N=454)被纳入荟萃分析。11 项研究中有 10 项研究的基线加权 PS 评分预测了 OS,PS 评分为 1.0 的患者的中位 OS 为 6.3 个月(95%后验区间为 5.4-7.4)。在调整基线 PS 后,FOLFOX 的治疗效果与氟尿嘧啶/亚叶酸联合纳米脂质体伊立替康治疗相似(中位 OS,2.6-6.7 个月)。中性粒细胞减少症和疲劳是与 FOLFOX 相关的最常见的 3-4 级 TRAEs。
当解释在一线吉西他滨为基础的治疗方案进展后的胰腺癌患者使用氟尿嘧啶和奥沙利铂治疗的疗效时,基线 PS 是一个强有力的预后因素。当考虑基线 PS 时,FOLFOX 与氟尿嘧啶和纳米脂质体伊立替康治疗具有相似的治疗效果和相似的安全性。这些发现表明,对于接受过吉西他滨治疗的体能状况良好(如 ECOG 0-1)的胰腺癌患者,氟尿嘧啶和奥沙利铂为基础的治疗仍然是一种可接受的替代二线治疗选择。