Department of Radiology, Yamaguchi University Graduate School of Medicine, 1-1-1 Minamikogushi, Ube, Yamaguchi, 755-8505, Japan.
Department of Radiology, National Hospital Organization, Yamaguchi-Ube Medical Center, 685 Higashikiwa, Ube, Yamaguchi, 755-0241, Japan.
Jpn J Radiol. 2023 Jan;41(1):27-37. doi: 10.1007/s11604-022-01328-4. Epub 2022 Sep 9.
To differentiate among infectious diseases, drug-induced lung injury (DILI) and pulmonary infiltration due to underlying malignancy (PIUM) based on high-resolution computed tomographic (HRCT) findings from patients with hematological malignancies who underwent chemotherapy or hematopoietic stem cell transplantation.
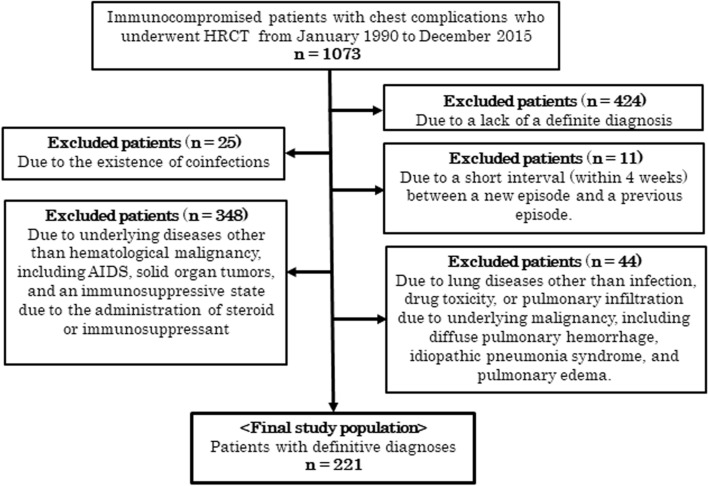
A total of 221 immunocompromised patients with hematological malignancies who had proven chest complications (141 patients with infectious diseases, 24 with DILI and 56 with PIUM) were included. Two chest radiologists evaluated the HRCT findings, including ground-glass opacity, consolidation, nodules, and thickening of bronchovascular bundles (BVBs) and interlobular septa (ILS). After comparing these CT findings among the three groups using the χtest, multiple logistic regression analyses (infectious vs noninfectious diseases, DILI vs non-DILI, and PIUM vs non-PIUM) were performed to detect useful indicators for differentiation.
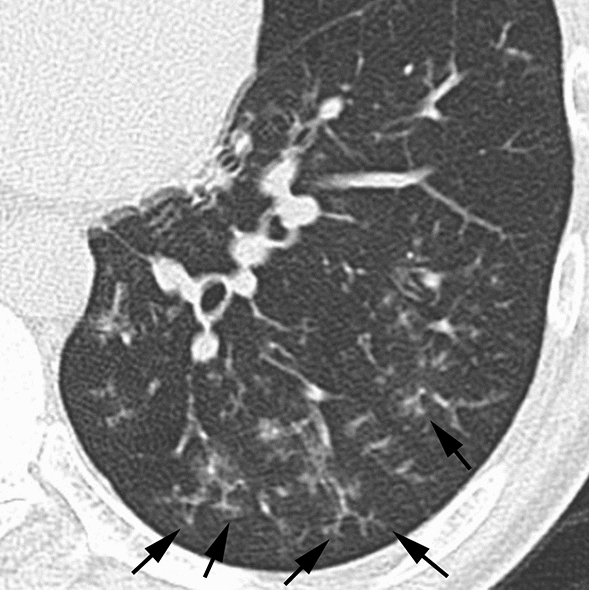
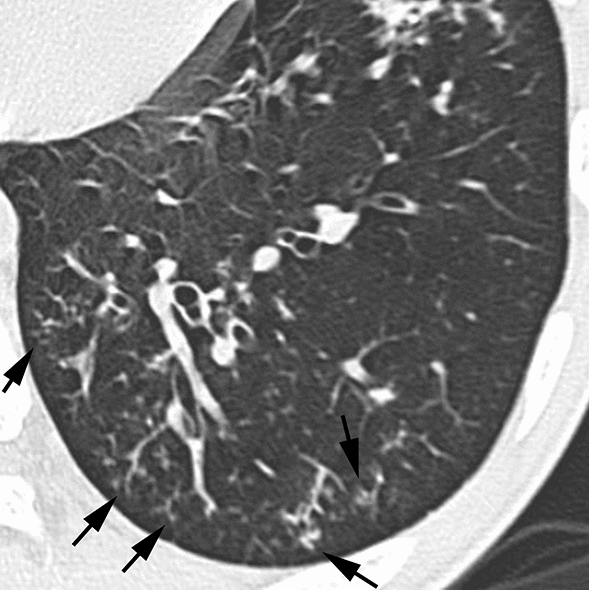
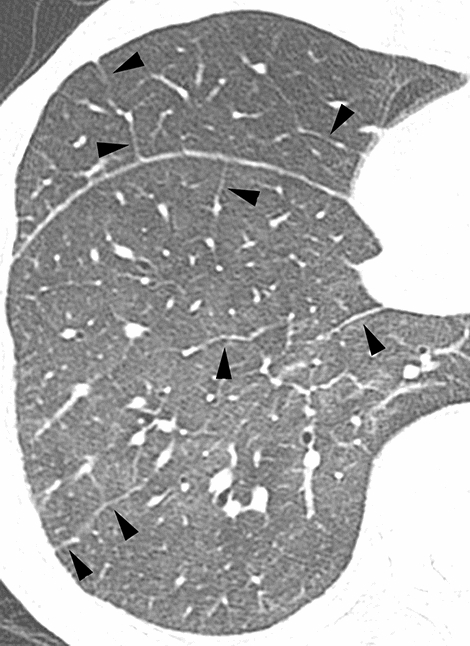
Significant differences were detected in many HRCT findings by the χ test. The results from the multiple logistic regression analyses identified several indicators: nodules without a perilymphatic distribution [p = 0.012, odds ratio (95% confidence interval): 4.464 (1.355-11.904)], nodules with a tree-in-bud pattern [p = 0.011, 8.364 (1.637-42.741)], and the absence of ILS thickening[p = 0.003, 3.621 (1.565-8.381)] for infectious diseases, the presence of ILS thickening [p = 0.001, 7.166 (2.343-21.915)] for DILI, and nodules with a perilymphatic distribution [p = 0.011, 4.256 (1.397-12.961)] and lymph node enlargement (p = 0.008, 3.420 (1.385-8.441)] for PIUM.
ILS thickening, nodules with a perilymphatic distribution, tree-in-bud pattern, and lymph node enlargement could be useful indicators for differentiating among infectious diseases, DILI, and PIUM in patients with hematological malignancies.
根据接受化疗或造血干细胞移植的血液恶性肿瘤患者的高分辨率计算机断层扫描(HRCT)结果,区分传染病、药物性肺损伤(DILI)和基础恶性肿瘤引起的肺部浸润(PIUM)。
共纳入 221 例有明确胸部并发症的免疫功能低下血液恶性肿瘤患者(141 例传染病,24 例 DILI,56 例 PIUM)。两位胸部放射科医生评估了 HRCT 发现,包括磨玻璃影、实变、结节以及支气管血管束(BVB)和小叶间隔(ILS)增厚。使用 χ 检验比较三组之间的这些 CT 发现后,进行了多变量逻辑回归分析(感染性与非感染性疾病、DILI 与非 DILI、PIUM 与非 PIUM),以检测有用的鉴别指标。
χ 检验发现许多 HRCT 发现存在显著差异。多变量逻辑回归分析的结果确定了几个指标:无淋巴管分布的结节(p=0.012,优势比[95%置信区间]:4.464[1.355-11.904])、树芽征结节(p=0.011,8.364[1.637-42.741])和无 ILS 增厚(p=0.003,3.621[1.565-8.381])提示为传染病,有 ILS 增厚(p=0.001,7.166[2.343-21.915])提示为 DILI,有淋巴管分布的结节(p=0.011,4.256[1.397-12.961])和淋巴结肿大(p=0.008,3.420[1.385-8.441])提示为 PIUM。
血液恶性肿瘤患者中,ILS 增厚、有淋巴管分布的结节、树芽征和淋巴结肿大可能是区分传染病、DILI 和 PIUM 的有用指标。