Clinic for Spine Surgery, Schoen-Clinic Hamburg, Academic Hospital of the University Medical Center Eppendorf, Dehnhaide 120, 22081, Hamburg, Germany.
CRO - Dr. med. Kottmann GmbH & Co. KG, Hamm, Germany.
Neuroradiology. 2022 Nov;64(11):2191-2201. doi: 10.1007/s00234-022-03047-z. Epub 2022 Sep 9.
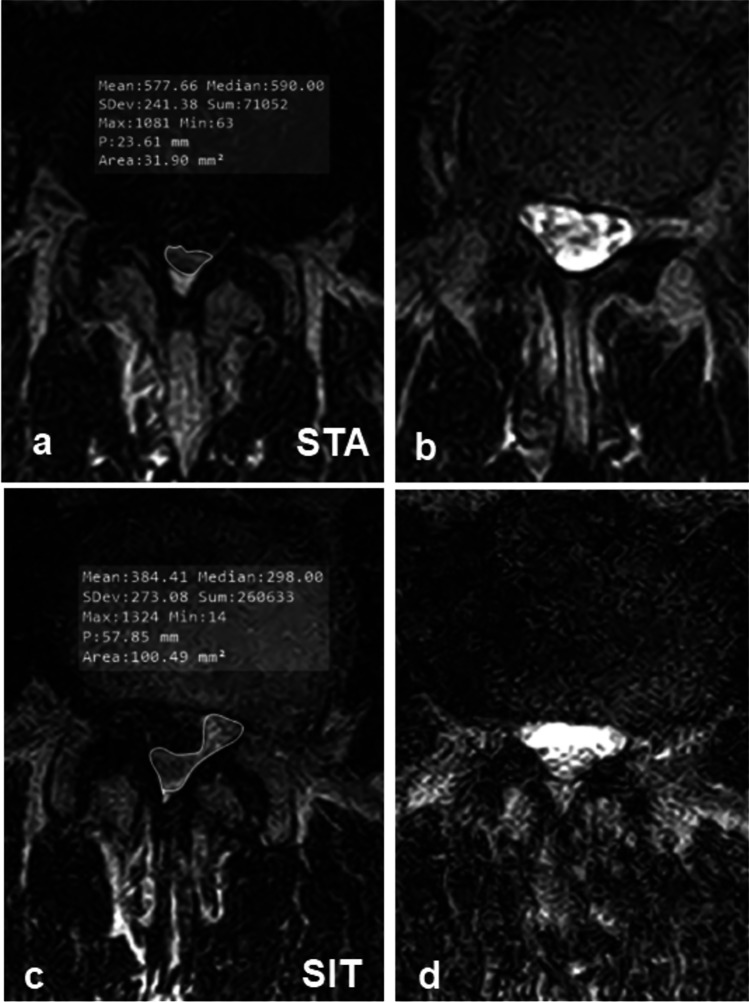
This retrospective cross-sectional cohort study investigated the influence of posture on lordosis (LL), length of the spinal canal (LSC), anteroposterior diameter (APD L1-L5), dural cross-sectional area (DCSA) of the lumbar spinal canal, and the prevalence of redundant nerve roots (RNR) using positional magnetic resonance imaging (MRI) (0.6 T).
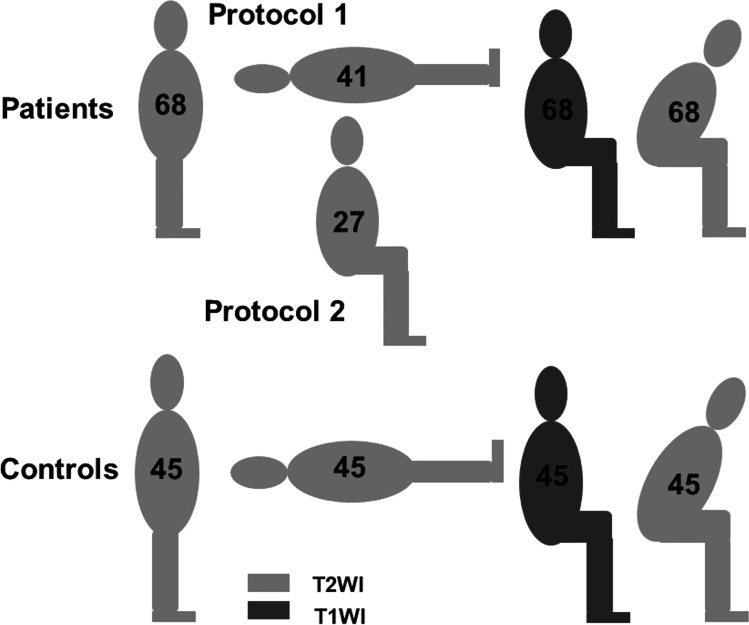
Sixty-eight patients with single-level degenerative central lumbar spinal stenosis (cLSS) presenting with RNR in the standing position (STA) were also investigated in supine (SUP) or neutral seated (SIT) and flexed seated (FLEX) positions. Additionally, 45 patients complaining of back pain and without MRI evidence of LSS were evaluated. Statistical significance was set at p < 0.05.
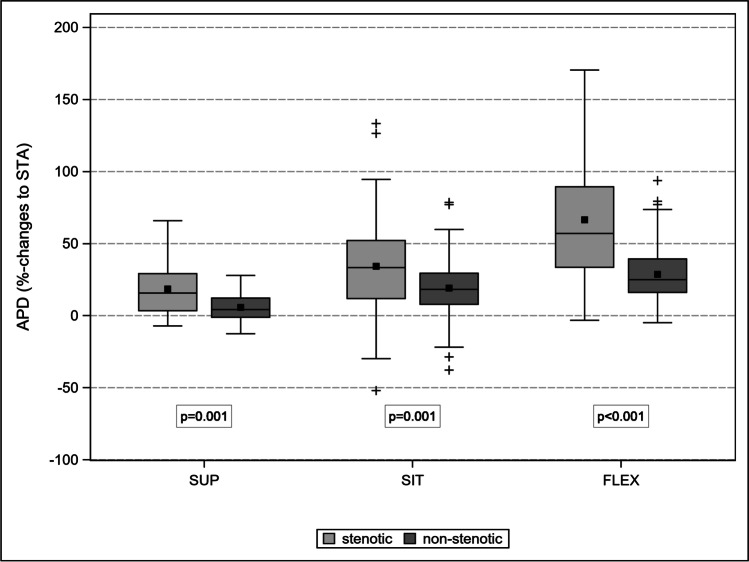
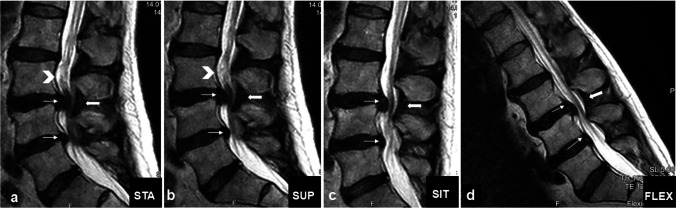
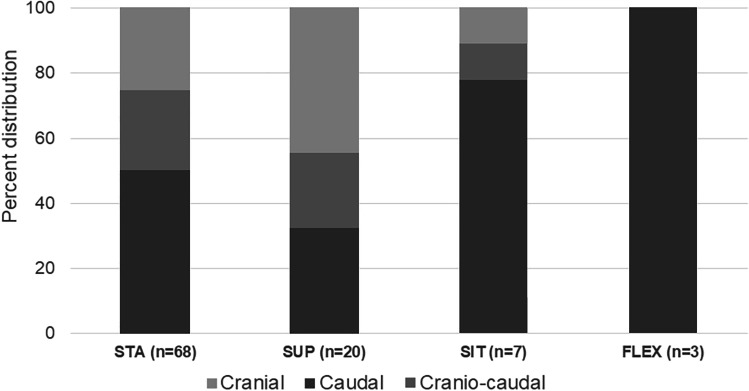
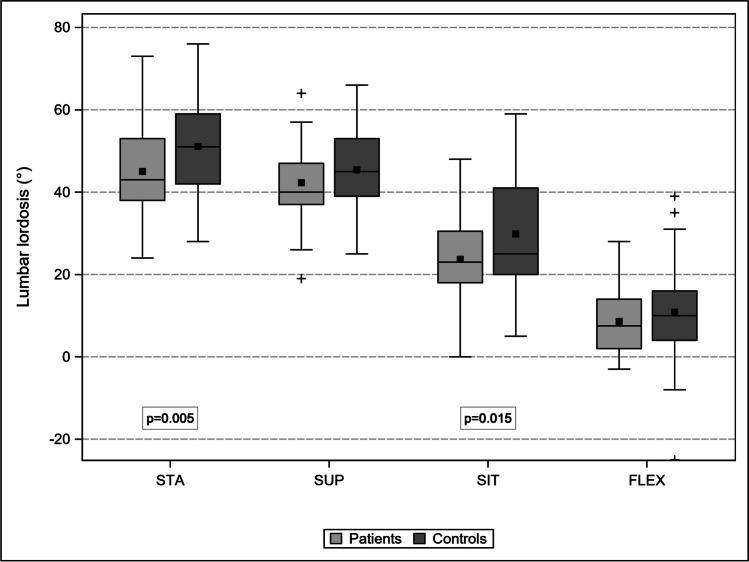
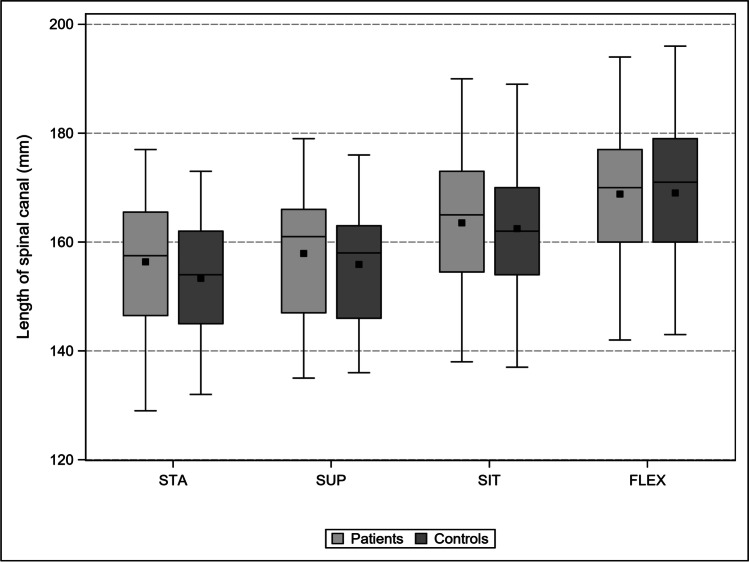
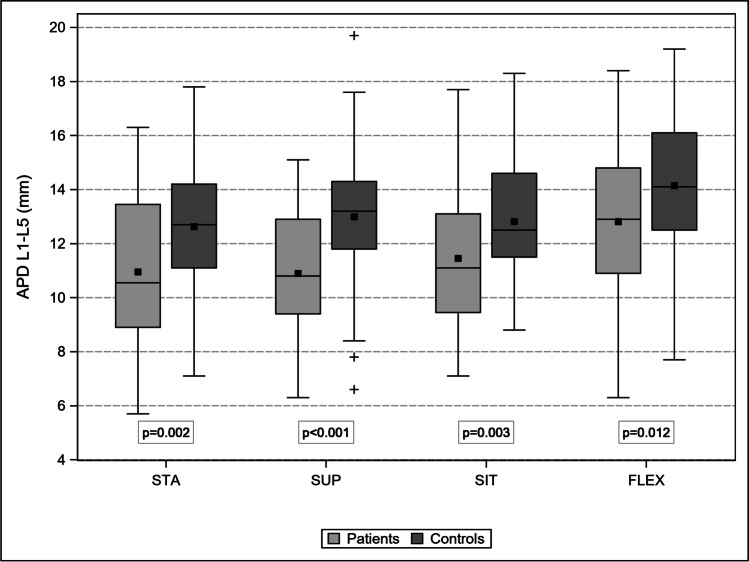
Controls (A) and patients with cLSS (B) were comparable in terms of mean age (p = 0.88) and sex (p = 0.22). The progressive transition from STA to FLEX led to a comparable decrease in LL (p = 0.97), an increase in LSC (p = 0.80), and an increase in APD L1-L5 (p = 0.78). The APD of the stenotic level increased disproportionally between the different postures, up to 67% in FLEX compared to 29% in adjacent non-stenotic levels (p < 0.001). Therefore, the prevalence of RNR decreased to 49, 26, and 4% in SUP, SIT, and FLEX, respectively.
The prevalence of RNR in standing position was underestimated by half in supine position. Body postures modified LL, LSC, and APD similarly in patients and controls. Stenotic levels compensated for insufficient intraspinal volume with a disproportionate enlargement when switching from the STA to FLEX.
本回顾性横断面队列研究旨在通过体位磁共振成像(0.6T)研究体位对腰椎前凸(LL)、椎管长度(LSC)、前后径(L1-L5 的 APD)、椎管硬脊膜横截面积(DCSA)以及冗余神经根(RNR)的发生率的影响。
本研究共纳入 68 例单节段退行性中央型腰椎管狭窄症(cLSS)患者,这些患者在站立位(STA)时存在 RNR,并在仰卧位(SUP)、中立位坐姿(SIT)和前屈位坐姿(FLEX)下进行检查。此外,还评估了 45 例腰痛但 MRI 未见 LSS 证据的患者。统计学意义设定为 p<0.05。
cLSS 患者(B)与对照组(A)在平均年龄(p=0.88)和性别(p=0.22)方面具有可比性。STA 到 FLEX 的逐步过渡导致 LL 相似下降(p=0.97)、LSC 相似增加(p=0.80)以及 L1-L5 的 APD 相似增加(p=0.78)。在不同的体位下,狭窄水平的 APD 不成比例地增加,与相邻非狭窄水平相比,FLEX 时增加了 67%,而在 STA 时仅增加了 29%(p<0.001)。因此,SUP、SIT 和 FLEX 时 RNR 的发生率分别下降至 49%、26%和 4%。
仰卧位时,站立位 RNR 的发生率被低估了一半。体位改变同样影响患者和对照组的 LL、LSC 和 APD。当从 STA 转换为 FLEX 时,狭窄水平通过不成比例的增大来补偿椎管内空间不足。