University of Turin, Department of Oncology, San Luigi University Hospital, Div of Surgical Oncology, Orbassano, Turin, Italy.
Department of Oncology, Head Surgical Oncology and Digestive Surgery, University of Torino, San Luigi University Hospital, Regione Gonzole 10 Orbassano, 10043, Turin, Italy.
Surg Endosc. 2023 Feb;37(2):977-988. doi: 10.1007/s00464-022-09547-6. Epub 2022 Sep 9.
Evidence on the efficacy of minimally invasive (MI) segmental resection of splenic flexure cancer (SFC) is not available, mostly due to the rarity of this tumor. This study aimed to determine the survival outcomes of MI and open treatment, and to investigate whether MI is noninferior to open procedure regarding short-term outcomes.
This nationwide retrospective cohort study included all consecutive SFC segmental resections performed in 30 referral centers between 2006 and 2016. The primary endpoint assessing efficacy was the overall survival (OS). The secondary endpoints included cancer-specific mortality (CSM), recurrence rate (RR), short-term clinical outcomes (a composite of Clavien-Dindo > 2 complications and 30-day mortality), and pathological outcomes (a composite of lymph nodes removed ≧12, and proximal and distal free resection margins length ≧ 5 cm). For these composites, a 6% noninferiority margin was chosen based on clinical relevance estimate.
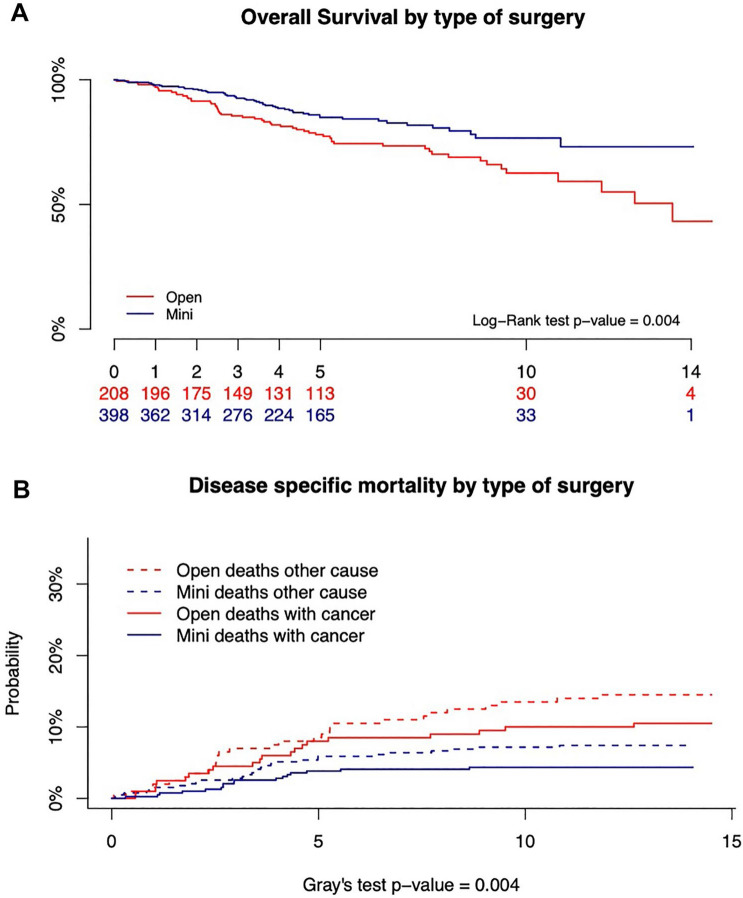
A total of 606 patients underwent either an open (208, 34.3%) or a MI (398, 65.7%) SFC segmental resection. At univariable analysis, OS and CSM were improved in the MI group (log-rank test p = 0.004 and Gray's tests p = 0.004, respectively), while recurrences were comparable (Gray's tests p = 0.434). Cox multivariable analysis did not support that OS and CSM were better in the MI group (p = 0.109 and p = 0.163, respectively). Successful pathological outcome, observed in 53.2% of open and 58.3% of MI resections, supported noninferiority (difference 5.1%; 1-sided 95%CI - 4.7% to ∞). Successful short-term clinical outcome was documented in 93.3% of Open and 93.0% of MI procedures, and supported noninferiority as well (difference - 0.3%; 1-sided 95%CI - 5.0% to ∞).
Among patients with SFC, the minimally invasive approach met the criterion for noninferiority for postoperative complications and pathological outcomes, and was found to provide results of OS, CSM, and RR comparable to those of open resection.
微创(MI)节段性切除脾曲结肠癌(SFC)的疗效证据尚不可用,主要是因为这种肿瘤很少见。本研究旨在确定 MI 和开放性治疗的生存结果,并探讨 MI 在短期结果方面是否不劣于开放性手术。
本项全国性回顾性队列研究纳入了 2006 年至 2016 年间在 30 个转诊中心进行的所有连续 SFC 节段切除术。评估疗效的主要终点是总生存率(OS)。次要终点包括癌症特异性死亡率(CSM)、复发率(RR)、短期临床结果(Clavien-Dindo 分级>2 级并发症和 30 天死亡率的复合指标)和病理结果(复合指标包括淋巴结切除数≧12 个、近端和远端无瘤切缘长度≧5cm)。对于这些复合指标,根据临床相关性估计选择了 6%的非劣效性边界。
共有 606 例患者接受了开放性(208 例,34.3%)或 MI(398 例,65.7%)SFC 节段切除术。单变量分析显示,MI 组的 OS 和 CSM 改善(对数秩检验 p=0.004 和 Gray 检验 p=0.004),而复发率相似(Gray 检验 p=0.434)。Cox 多变量分析不支持 MI 组的 OS 和 CSM 更好(p=0.109 和 p=0.163)。在开放和 MI 切除术中分别观察到 53.2%和 58.3%的成功病理结果,支持非劣效性(差异 5.1%;单侧 95%CI-4.7%至∞)。93.3%的开放性手术和 93.0%的 MI 手术记录了成功的短期临床结果,也支持非劣效性(差异-0.3%;单侧 95%CI-5.0%至∞)。
在 SFC 患者中,微创方法符合术后并发症和病理结果非劣效性标准,并且发现 OS、CSM 和 RR 的结果与开放性切除相当。