Reiter Anna, De Meulemeester Julie, Kenya-Mugisha Nathan, Tagoola Abner, Kabajaasi Olive, Wiens Matthew O, Duby Jessica
Faculty of Medicine and Health Sciences, McGill University, Montreal, QC, Canada.
Walimu, Kampala, Uganda.
Front Pediatr. 2022 Aug 25;10:987228. doi: 10.3389/fped.2022.987228. eCollection 2022.
To determine the effect of parental participation in hospital care on neonatal and parental outcomes in low- and middle-income countries (LMICs) and to identify the range of parental duties in the care of hospitalized neonates in LMICs.
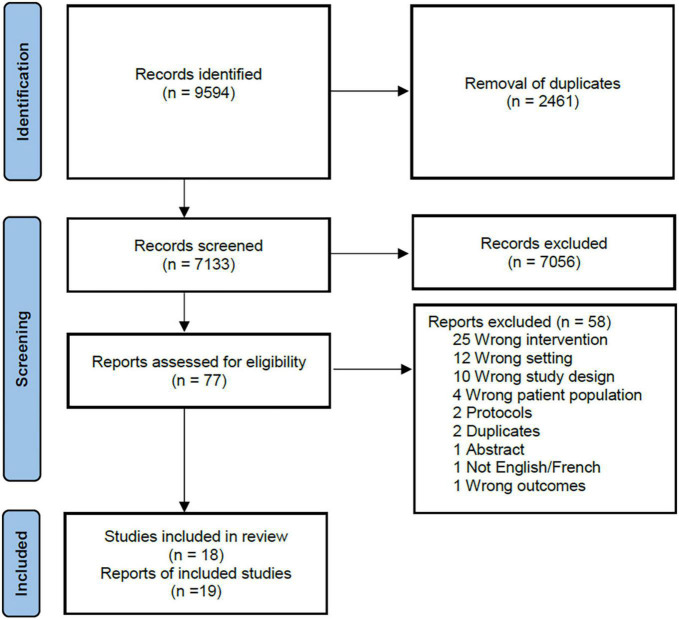
We searched CINAHL, CENTRAL, LILACs, MEDLINE, EMBASE and Web of Science from inception to February 2022. Randomized and non-randomized studies from LMICs were eligible if parents performed one or more roles traditionally undertaken by healthcare staff. The primary outcome was hospital length-of-stay. Secondary outcomes included mortality, readmission, breastfeeding, growth, development and parental well-being. Data was extracted in duplicate by two independent reviewers using a piloted extraction form.
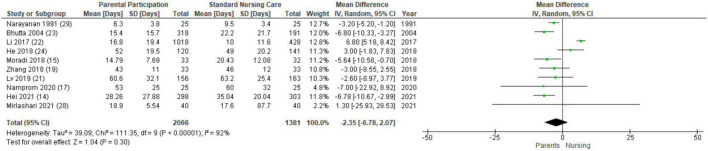
Eighteen studies (eight randomized and ten non-randomized) were included from seven middle-income countries. The types of parental participation included hygiene and infection prevention, feeding, monitoring and documentation, respiratory care, developmental care, medication administration and decision making. Meta-analyses showed that parental participation was not associated with hospital length-of-stay (MD -2.35, 95% CI -6.78-2.07). However, parental involvement was associated with decreased mortality (OR 0.46, 95% CI 0.22-0.95), increased breastfeeding (OR 2.97 95% CI 1.65-5.35) and decreased hospital readmission (OR 0.36, 95% CI 0.16-0.81). Narrative synthesis demonstrated additional benefits for growth, short-term neurodevelopment and parental well-being. Ten of the eighteen studies had a high risk of bias.
Parental participation in neonatal hospital care is associated with improvement in several key neonatal outcomes in middle-income countries. The lack of data from low-income countries suggests that there remains barriers to parental participation in resource-poor settings.
[https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=187562], identifier [CRD42020187562].
确定在低收入和中等收入国家(LMICs)中,父母参与医院护理对新生儿及父母结局的影响,并确定LMICs中父母在照顾住院新生儿方面的职责范围。
我们检索了从数据库建立至2022年2月的CINAHL、CENTRAL、LILACs、MEDLINE、EMBASE和Web of Science数据库。如果父母承担了一项或多项传统上由医护人员承担的职责,则来自LMICs的随机和非随机研究均符合条件。主要结局是住院时间。次要结局包括死亡率、再入院率、母乳喂养、生长发育、父母幸福感。两名独立评审员使用预先测试的提取表对数据进行了重复提取。
纳入了来自七个中等收入国家的18项研究(8项随机研究和10项非随机研究)。父母参与的类型包括卫生和感染预防、喂养、监测和记录、呼吸护理、发育护理、药物管理和决策。荟萃分析表明,父母参与与住院时间无关(MD -2.3
5,95% CI -6.78 - 2.07)。然而,父母参与与死亡率降低(OR 0.46,95% CI 0.22 - 0.95)、母乳喂养增加(OR 2.97,95% CI 1.65 - 5.35)和医院再入院率降低(OR 0.36,95% CI 0.16 - 0.81)相关。叙述性综合分析表明,对生长发育、短期神经发育和父母幸福感还有其他益处。18项研究中有10项存在高偏倚风险。
在中等收入国家,父母参与新生儿医院护理与改善多项关键新生儿结局相关。低收入国家缺乏数据表明,在资源匮乏的环境中,父母参与仍然存在障碍。
[https://www.crd.york.ac.uk/prospero/display_record.php?RecordID=187562],标识符[CRD42020187562]。