Hou Yuanzheng, Li Ye, Li Qiongge, Yu Yang, Tang Jie
Department of Neurosurgery, Xuanwu Hospital, Capital Medical University, Beijing, China.
Department of Radiology, Xuanwu Hospital, Capital Medical University, Beijing, China.
Front Oncol. 2022 Aug 25;12:955807. doi: 10.3389/fonc.2022.955807. eCollection 2022.
Intraoperative ultrasound(iUS) and intraoperative MRI (iMRI) are effective ways to perform resection control during glioma surgery. However, most published studies employed only one modality. Few studies have used both during surgery. How to combine these two techniques reasonably, and what advantages they could have for glioma surgery are still open questions.
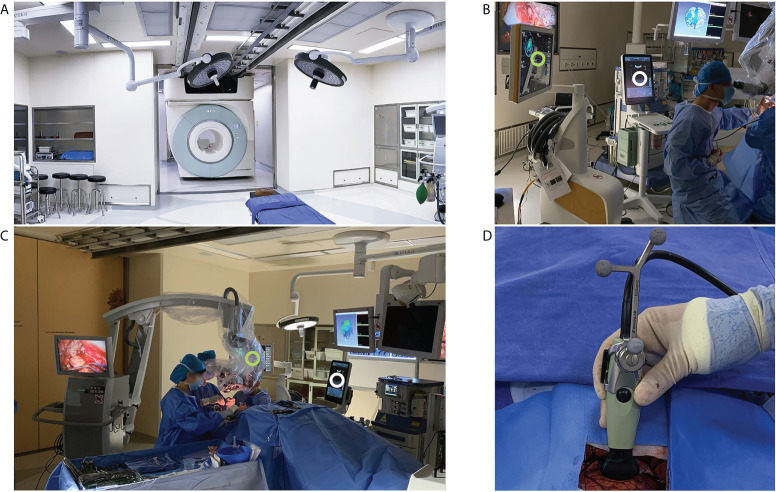
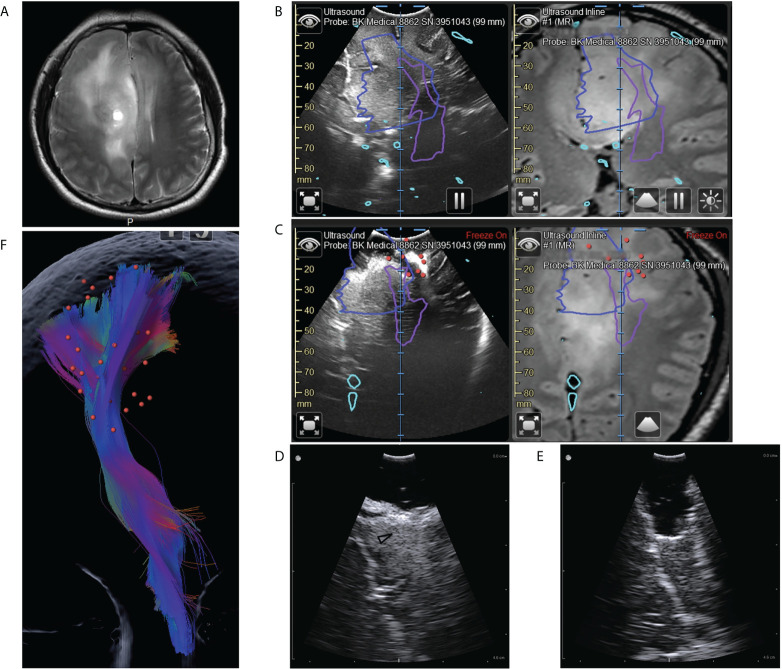
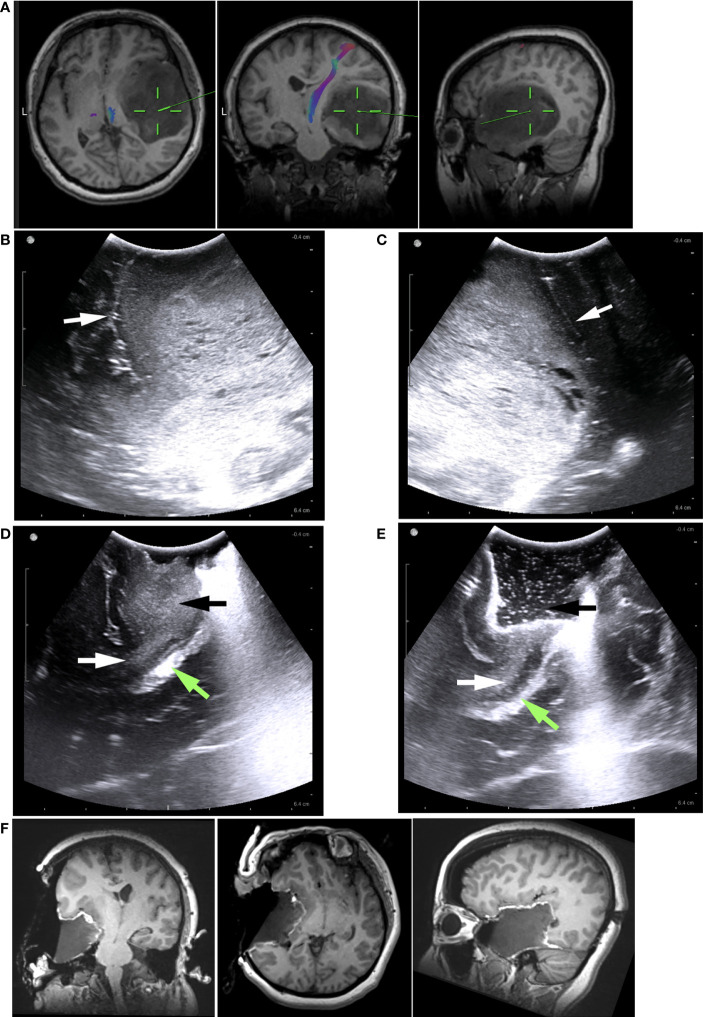
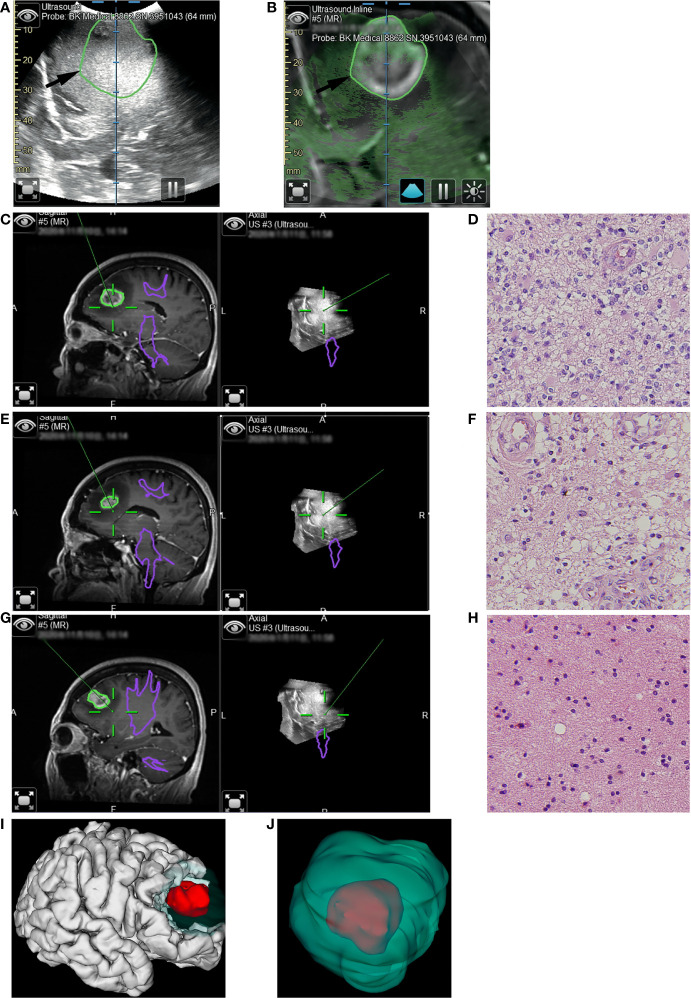
We retrospectively reviewed a series of consecutive patients who underwent initial surgical treatment of supratentorial gliomas in our center. We utilized a full-course resection control strategy to combine iUS and iMRI: IUS for pre-resection assessment and intermediate resection control; iMRI for final resection control. The basic patient characteristics, surgical results, iMRI/iUS findings, and their impacts on surgical procedures were evaluated and reported.
A total of 40 patients were included. The extent of resection was 95.43 ± 10.37%, and the gross total resection rate was 72.5%. The median residual tumor size was 6.39 cm (range 1.06-16.23 cm3). 5% (2/40) of patients had permanent neurological deficits after surgery. 17.5% (7/40) of patients received further resection after the first iMRI scan, resulting in four (10%) more patients achieving gross total resection. The number of iMRI scans per patient was 1.18 ± 0.38. The surgical time was 4.5 ± 3.6 hours. The pre-resection iUS scan revealed that an average of 3.8 borders of the tumor were beside sulci in 75% (30/40) patients. Intermediate resection control was utilized in 67.5% (27/40) of patients. In 37.5% (15/40) of patients, the surgical procedures were changed intraoperatively based on the iUS findings. Compared with iMRI, the sensitivity and specificity of iUS for residual tumors were 46% and 96%, respectively.
The full-course resection control strategy by combining iUS and iMRI could be successfully implemented with good surgical results in initial glioma surgeries. This strategy might stabilize resection control quality and provide the surgeon with more intraoperative information to tailor the surgical strategy. Compared with iMRI-assisted glioma surgery, this strategy might improve efficiency by reducing the number of iMRI scans and shortening surgery time.
术中超声(iUS)和术中磁共振成像(iMRI)是胶质瘤手术中进行切除控制的有效方法。然而,大多数已发表的研究仅采用了一种方式。很少有研究在手术中同时使用这两种方法。如何合理结合这两种技术,以及它们对胶质瘤手术有哪些优势,仍然是悬而未决的问题。
我们回顾性分析了在本中心接受幕上胶质瘤初次手术治疗的一系列连续患者。我们采用全程切除控制策略将iUS和iMRI相结合:iUS用于切除前评估和中间切除控制;iMRI用于最终切除控制。对患者的基本特征、手术结果、iMRI/iUS检查结果及其对手术过程的影响进行了评估和报告。
共纳入40例患者。切除范围为95.43±10.37%,全切率为72.5%。残余肿瘤大小中位数为6.39 cm(范围1.06 - 16.23 cm³)。5%(2/40)的患者术后出现永久性神经功能缺损。17.5%(7/40)的患者在首次iMRI扫描后接受了进一步切除,使全切患者增加了4例(10%)。每位患者的iMRI扫描次数为1.18±0.38次。手术时间为4.5±3.6小时。切除前iUS扫描显示,75%(30/40)的患者肿瘤平均有3.8个边界位于脑沟旁。67.5%(27/40)的患者采用了中间切除控制。37.5%(15/40)的患者术中根据iUS检查结果改变了手术方式。与iMRI相比,iUS对残余肿瘤的敏感性和特异性分别为46%和96%。
在初次胶质瘤手术中,通过结合iUS和iMRI的全程切除控制策略可以成功实施,并取得良好的手术效果。该策略可能稳定切除控制质量,并为外科医生提供更多术中信息以调整手术策略。与iMRI辅助的胶质瘤手术相比,该策略可能通过减少iMRI扫描次数和缩短手术时间来提高效率。