Neurosurgery and Neurooncology Service, Centre Hospitalier Regional Universitaire de Lille, Roger Salengro Hospital, Lille, France.
Department of Clinical Neurosciences, Neurosurgery Service and Gamma Knife Center, Lausanne University Hospital (CHUV), Lausanne, Switzerland.
Neurosurg Rev. 2021 Dec;44(6):2977-2990. doi: 10.1007/s10143-021-01488-3. Epub 2021 Feb 3.
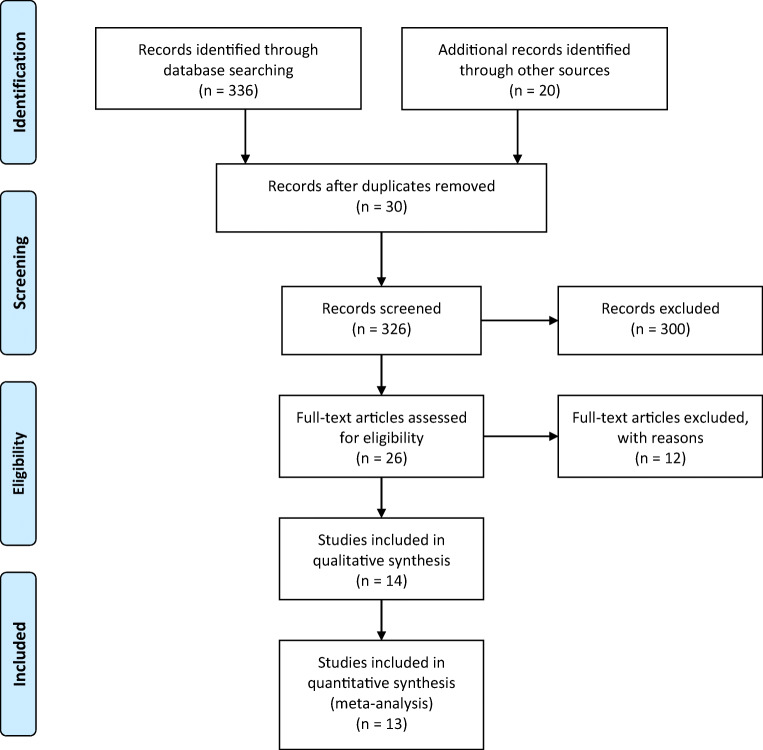
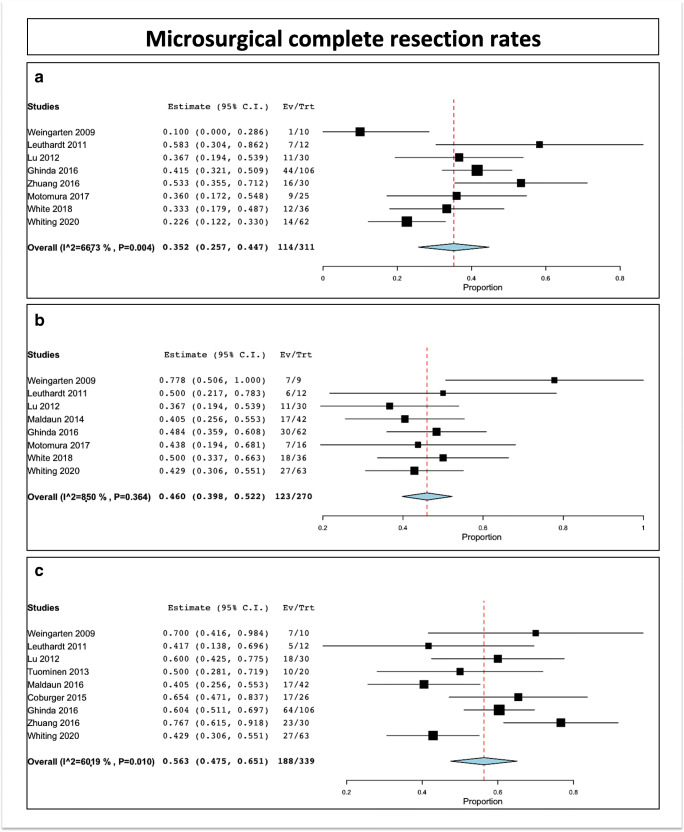
Microsurgical resection of primary brain tumors located within or near eloquent areas is challenging. Primary aim is to preserve neurological function, while maximizing the extent of resection (EOR), to optimize long-term neurooncological outcomes and quality of life. Here, we review the combined integration of awake craniotomy and intraoperative MRI (IoMRI) for primary brain tumors, due to their multiple challenges. A systematic review of the literature was performed, in accordance with the Prisma guidelines. Were included 13 series and a total number of 527 patients, who underwent 541 surgeries. We paid particular attention to operative time, rate of intraoperative seizures, rate of initial complete resection at the time of first IoMRI, the final complete gross total resection (GTR, complete radiological resection rates), and the immediate and definitive postoperative neurological complications. The mean duration of surgery was 6.3 h (median 7.05, range 3.8-7.9). The intraoperative seizure rate was 3.7% (range 1.4-6; I^2 = 0%, P heterogeneity = 0.569, standard error = 0.012, p = 0.002). The intraoperative complete resection rate at the time of first IoMRI was 35.2% (range 25.7-44.7; I^2 = 66.73%, P heterogeneity = 0.004, standard error = 0.048, p < 0.001). The rate of patients who underwent supplementary resection after one or several IoMRI was 46% (range 39.8-52.2; I^2 = 8.49%, P heterogeneity = 0.364, standard error = 0.032, p < 0.001). The GTR rate at discharge was 56.3% (range 47.5-65.1; I^2 = 60.19%, P heterogeneity = 0.01, standard error = 0.045, p < 0.001). The rate of immediate postoperative complications was 27.4% (range 15.2-39.6; I^2 = 92.62%, P heterogeneity < 0.001, standard error = 0.062, p < 0.001). The rate of permanent postoperative complications was 4.1% (range 1.3-6.9; I^2 = 38.52%, P heterogeneity = 0.123, standard error = 0.014, p = 0.004). Combined use of awake craniotomy and IoMRI can help in maximizing brain tumor resection in selected patients. The technical obstacles to doing so are not severe and can be managed by experienced neurosurgery and anesthesiology teams. The benefits of bringing these technologies to bear on patients with brain tumors in or near language areas are obvious. The lack of equipoise on this topic by experienced practitioners will make it difficult to do a prospective, randomized, clinical trial. In the opinion of the authors, such a trial would be unnecessary and would deprive some patients of the benefits of the best available methods for their tumor resections.
在功能区或功能区附近的原发性脑肿瘤的显微外科切除具有挑战性。主要目标是在最大程度保留神经功能的同时,最大限度地提高肿瘤全切除程度(EOR),以优化长期神经肿瘤学结果和生活质量。在这里,我们回顾了由于具有多种挑战,因此将清醒开颅术和术中磁共振成像(IoMRI)相结合用于原发性脑肿瘤的情况。根据 Prisma 指南进行了文献的系统回顾。共纳入了 13 项系列研究和总共 527 例患者,这些患者共进行了 541 次手术。我们特别注意手术时间、术中癫痫发作率、首次 IoMRI 时初始完全切除率、最终完全大体全切(GTR,完全放射学切除率)以及即刻和确定性术后神经并发症。手术的平均持续时间为 6.3 小时(中位数为 7.05,范围为 3.8-7.9)。术中癫痫发作率为 3.7%(范围为 1.4-6;I^2 = 0%,P 异质性 = 0.569,标准误差 = 0.012,p = 0.002)。首次 IoMRI 时的术中完全切除率为 35.2%(范围为 25.7-44.7;I^2 = 66.73%,P 异质性 = 0.004,标准误差 = 0.048,p <0.001)。在一次或多次 IoMRI 后接受补充切除的患者比例为 46%(范围为 39.8-52.2;I^2 = 8.49%,P 异质性 = 0.364,标准误差 = 0.032,p <0.001)。出院时的 GTR 率为 56.3%(范围为 47.5-65.1;I^2 = 60.19%,P 异质性 = 0.01,标准误差 = 0.045,p <0.001)。即刻术后并发症的发生率为 27.4%(范围为 15.2-39.6;I^2 = 92.62%,P 异质性 <0.001,标准误差 = 0.062,p <0.001)。永久性术后并发症的发生率为 4.1%(范围为 1.3-6.9;I^2 = 38.52%,P 异质性 = 0.123,标准误差 = 0.014,p = 0.004)。清醒开颅术和 IoMRI 的联合使用可以帮助选定的患者最大限度地切除脑肿瘤。这样做的技术障碍并不严重,经验丰富的神经外科和麻醉科团队可以加以管理。将这些技术应用于语言区或语言区附近的脑肿瘤患者的益处是显而易见的。有经验的从业者在这个问题上缺乏平衡,这将使得很难进行前瞻性,随机的临床试验。作者认为,这样的试验是不必要的,并且会使某些患者失去其肿瘤切除的最佳可用方法的益处。