Cai Shaoyan, Wang Qinjia, Ma Chuzhou, Chen Junheng, Wei Yang, Zhang Lei, Fang Zengqiang, Zheng Liangjie, Guo Chunming
Department of Anesthesiology, Shantou Central Hospital, Shantou, China.
Department of Gastroenterology, The First Affiliated Hospital of Shantou University, Shantou, China.
Front Med (Lausanne). 2022 Aug 24;9:922280. doi: 10.3389/fmed.2022.922280. eCollection 2022.
This study aimed to evaluate the association between the glucose-to-lymphocyte ratio (GLR) and in-hospital mortality in intensive care unit (ICUs) patients with sepsis.
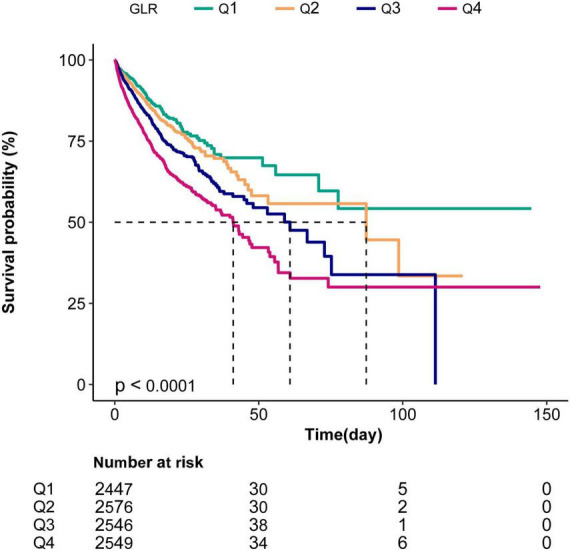
This is a retrospective cohort study. Patients with sepsis from the Medical Information Mart for Intensive Care-IV (MIMIC-IV) database had their baseline data and in-hospital prognosis retrieved. Multivariable Cox regression analyses were applied to calculate adjusted hazard ratios (HR) with 95% confidence intervals (CI). Survival curves were plotted, and subgroup analyses were stratified by relevant covariates. To address the non-linearity relationship, curve fitting and a threshold effect analysis were performed.
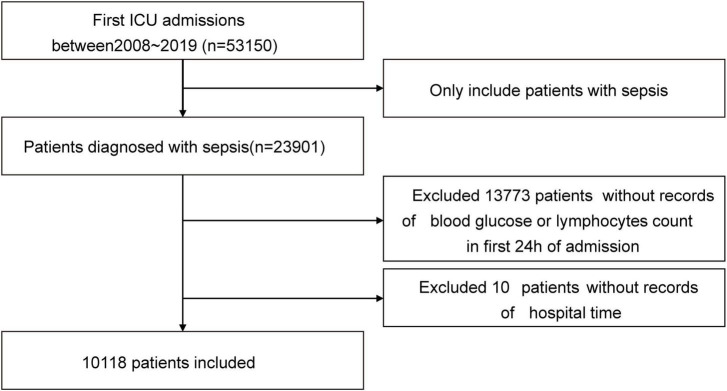
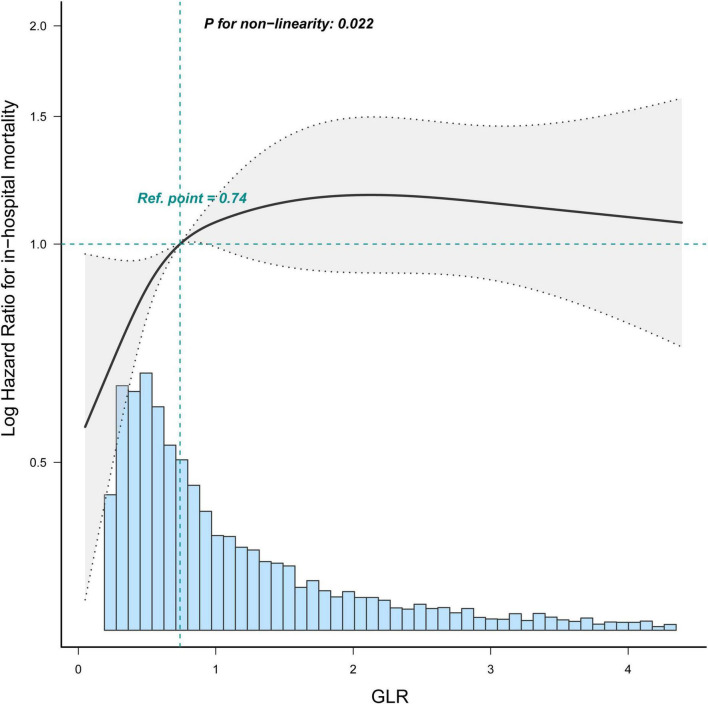
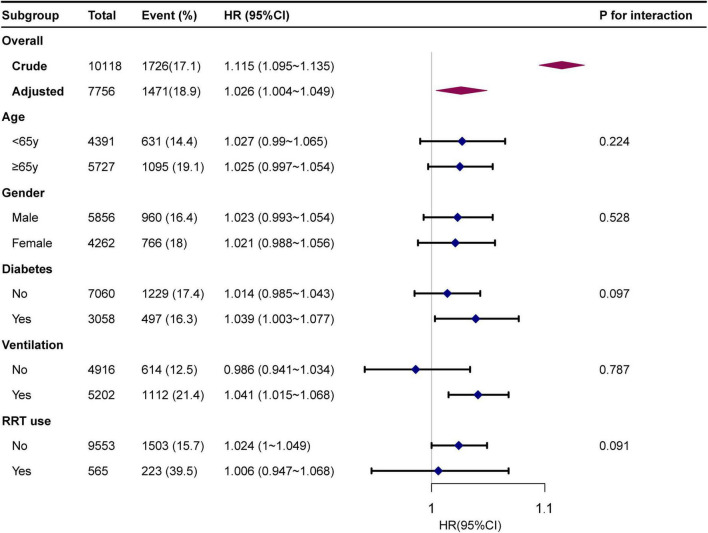
Of the 23,901 patients, 10,118 patients with sepsis were included. The overall in-hospital mortality rate was 17.1% (1,726/10,118). Adjusted for confounding factors in the multivariable Cox regression analysis models, when GLR was used as a categorical variable, patients in the highest GLR quartile had increased in-hospital mortality compared to patients in the lowest GLR quartile (HR = 1.26, 95% CI: 1.15-1.38). When GLR was used as a continuous variable, each unit increase in GLR was associated with a 2% increase in the prevalence of in-hospital mortality (adjusted HR = 1.02, 95% CI: 1.01-1.03, = 0.001). Stratified analyses indicated that the correlation between the GLR and in-hospital mortality was stable. The non-linear relationship between GLR and in-hospital mortality was explored in a dose-dependent manner. In-hospital mortality increased by 67% (aHR = 1.67, 95% CI: 1.45-1.92) for every unit GLR increase. When GLR was beyond 1.68, in-hospital mortality did not significantly change (aHR: 1.04, 95% CI: 0.92-1.18).
There is a non-linear relationship between GLR and in-hospital mortality in intensive care patients with sepsis. A higher GLR in ICU patients is associated with in-hospital mortality in the United States. However, further research is needed to confirm the findings.
本研究旨在评估脓毒症重症监护病房(ICU)患者的血糖与淋巴细胞比值(GLR)与院内死亡率之间的关联。
这是一项回顾性队列研究。从重症医学信息集市 - 第四版(MIMIC - IV)数据库中获取脓毒症患者的基线数据和院内预后。应用多变量Cox回归分析计算调整后的风险比(HR)及95%置信区间(CI)。绘制生存曲线,并按相关协变量进行亚组分析。为解决非线性关系,进行曲线拟合和阈值效应分析。
在23,901例患者中,纳入了10,118例脓毒症患者。总体院内死亡率为17.1%(1,726 / 10,118)。在多变量Cox回归分析模型中对混杂因素进行调整后,当GLR作为分类变量时,GLR最高四分位数的患者与GLR最低四分位数的患者相比,院内死亡率增加(HR = 1.26,95% CI:1.15 - 1.38)。当GLR作为连续变量时,GLR每增加一个单位,院内死亡率患病率增加2%(调整后HR = 1.02,95% CI:1.01 - 1.03,P = 0.001)。分层分析表明GLR与院内死亡率之间的相关性是稳定的。以剂量依赖方式探索了GLR与院内死亡率之间的非线性关系。GLR每增加一个单位,院内死亡率增加67%(调整后HR = 1.67,95% CI:1.45 - 1.92)。当GLR超过1.68时,院内死亡率无显著变化(调整后HR:1.04,95% CI:0.92 - 1.18)。
脓毒症重症监护患者的GLR与院内死亡率之间存在非线性关系。在美国,ICU患者中较高的GLR与院内死亡率相关。然而,需要进一步研究来证实这些发现。