Royston Léna, Isnard Stéphane, Perrin Nils, Sinyavskaya Liliya, Berini Carolina, Lin John, Trottier Benoit, Baril Jean-Guy, Chartrand-Lefebvre Carl, Tremblay Cecile, Durand Madeleine, Routy Jean-Pierre
Infectious Diseases and Immunity in Global Health Program, Research Institute, McGill University Health Centre, Montreal, QC, Canada.
Chronic Viral Illness Service, McGill University Health Centre, Montreal, QC, Canada.
Front Cardiovasc Med. 2022 Aug 26;9:964650. doi: 10.3389/fcvm.2022.964650. eCollection 2022.
Increased rates of cardiovascular diseases (CVD) and larger subclinical high-risk coronary plaques in coronary CT angiography have been observed in people living with HIV (PLWH) treated with antiretroviral therapy (ART) compared to HIV-uninfected people. Growth differentiation factor-15 (GDF-15) is a cytokine emerging as an optimal marker for CVD in the general population.
We cross-sectionally analyzed plasma of 95 PLWH on ART and 52 controls. We measured GDF-15, fibroblast growth factor-21 (FGF-21), glucagon-like peptide-2 (GLP-2), soluble urokinase plasminogen activator receptor (suPAR), CRP, and anti-CMV and anti-EBV IgG levels. All participants had no clinical CVD and underwent coronary CT angiography with the 3D reconstruction of coronary artery atherosclerotic plaques. Total plaque volume (TPV) and low attenuation plaque volume (LAPV, defined as density <30 Hounsfield Units) were calculated (mm).
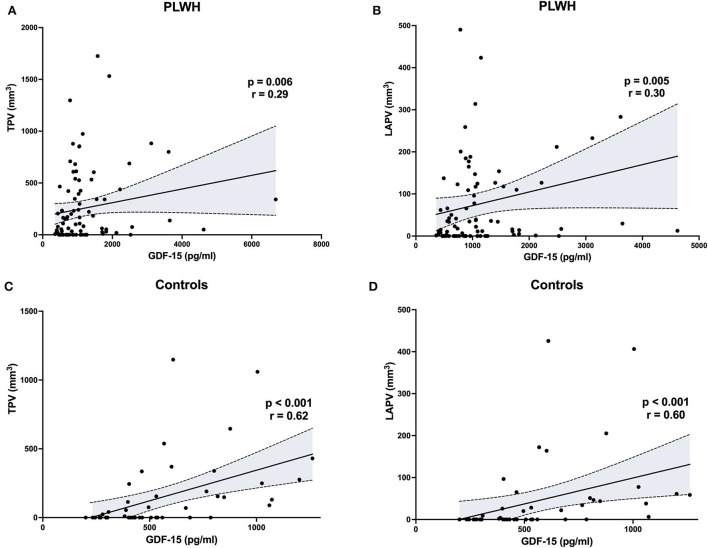
In both PLWH and controls, GDF-15 levels were increased in participants with presence of coronary plaque vs. without ( = 0.04 and < 0.001, respectively) and correlated with TPV ( = 0.27, = 0.009 and = 0.62, < 0.001, respectively) and LAPV ( = 0.28, = 0.008, = 0.60, < 0.001, respectively). However, in a multivariate model, GDF-15 was independently associated with LAPV in controls only (adjusted OR 35.1, = 0.04) and not in PLWH, mainly due to confounding by smoking. Other markers were not independently associated with plaque volume, except for anti-EBV IgGs in controls (adjusted OR 3.51, = 0.02).
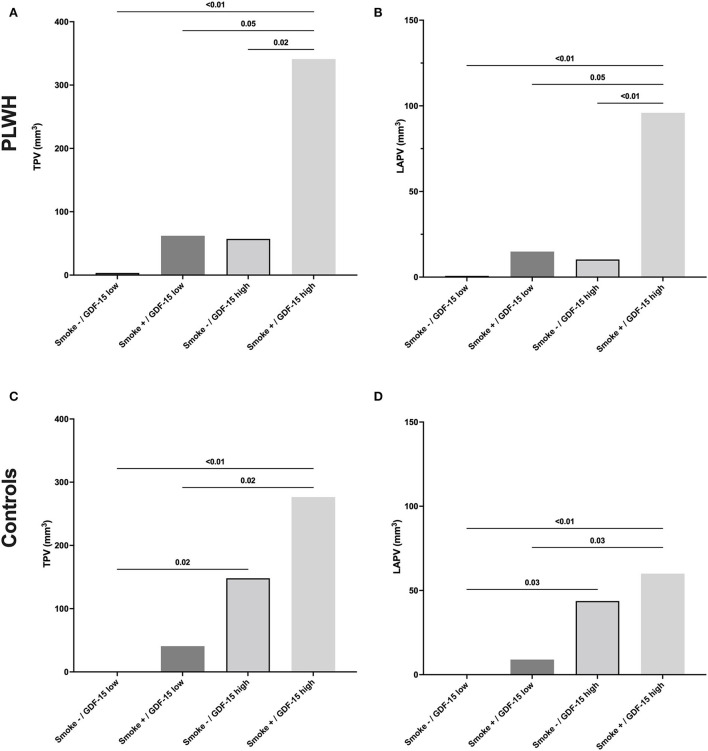
In PLWH, GDF-15 and smoking seemed to synergistically contribute to coronary plaque volume. Conversely, increased GDF-15 levels were associated with the presence of coronary artery plaques in people without HIV, independently of CV risk factors.
与未感染艾滋病毒的人相比,接受抗逆转录病毒疗法(ART)治疗的艾滋病毒感染者(PLWH)心血管疾病(CVD)发生率增加,且冠状动脉CT血管造影显示其亚临床高危冠状动脉斑块更大。生长分化因子-15(GDF-15)是一种细胞因子,已成为普通人群中CVD的最佳标志物。
我们对95例接受ART治疗的PLWH和52例对照者的血浆进行了横断面分析。我们测量了GDF-15、成纤维细胞生长因子-21(FGF-21)、胰高血糖素样肽-2(GLP-2)、可溶性尿激酶型纤溶酶原激活剂受体(suPAR)、CRP以及抗巨细胞病毒(CMV)和抗EB病毒IgG水平。所有参与者均无临床CVD,并接受了冠状动脉CT血管造影及冠状动脉粥样硬化斑块的三维重建。计算总斑块体积(TPV)和低密度斑块体积(LAPV,定义为密度<30亨氏单位)(mm)。
在PLWH和对照者中,有冠状动脉斑块的参与者的GDF-15水平均高于无斑块者(分别为P = 0.04和P < 0.001),且与TPV相关(分别为r = 0.27,P = 0.009和r = 0.62,P < 0.001)以及LAPV相关(分别为r = 0.28,P = 0.008,r = 0.60,P < 0.001)。然而,在多变量模型中,GDF-15仅在对照者中与LAPV独立相关(调整后的OR为35.1,P = 0.04),而在PLWH中并非如此,主要是由于吸烟的混杂作用。除对照者中的抗EB病毒IgG外(调整后的OR为3.51,P = 0.02),其他标志物与斑块体积均无独立相关性。
在PLWH中,GDF-15和吸烟似乎协同作用于冠状动脉斑块体积。相反,在未感染艾滋病毒的人中,GDF-15水平升高与冠状动脉斑块的存在相关,且独立于心血管危险因素。