University of California, San Francisco, CA.
Stanford Cancer Institute/Stanford University School of Medicine, Stanford, CA.
Blood Adv. 2023 May 9;7(9):1713-1724. doi: 10.1182/bloodadvances.2022008292.
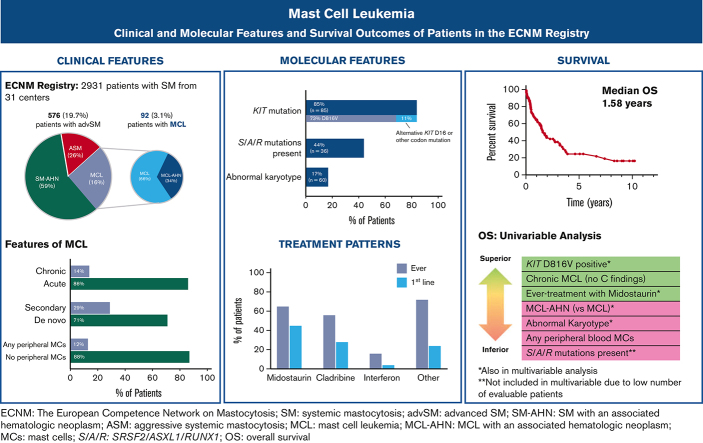
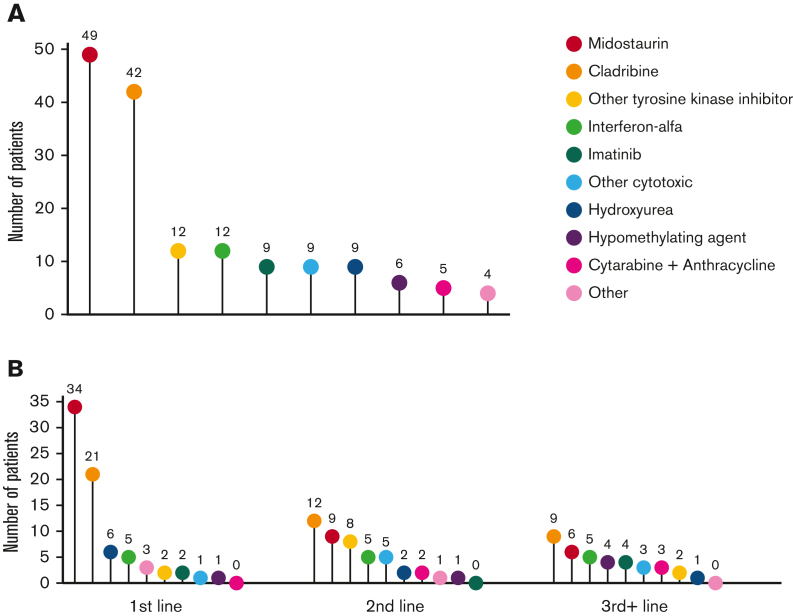
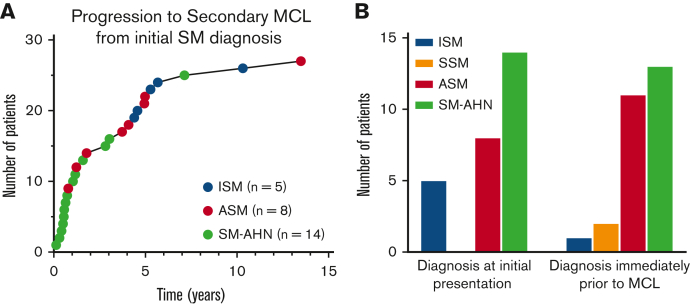
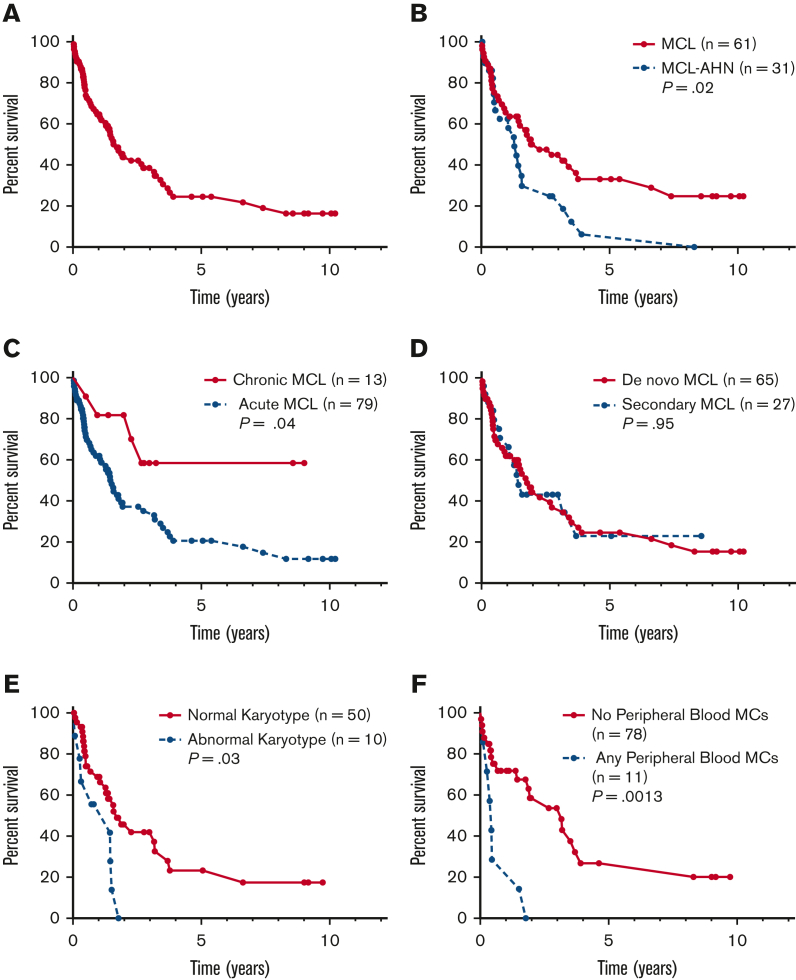
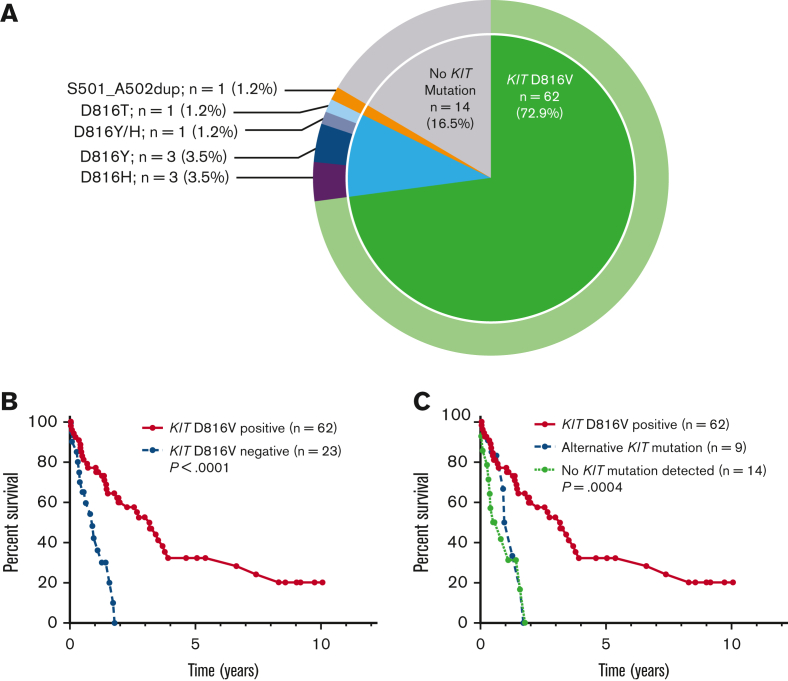
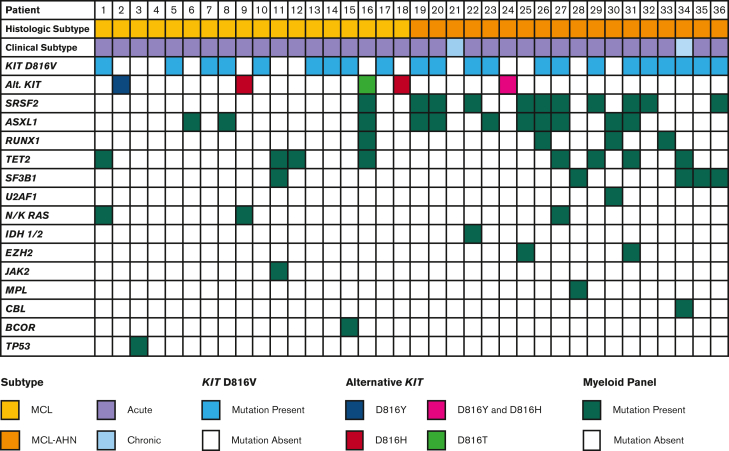
Mast cell leukemia (MCL) is a rare subtype of systemic mastocytosis defined by ≥20% mast cells (MC) on a bone marrow aspirate. We evaluated 92 patients with MCL from the European Competence Network on Mastocytosis registry. Thirty-one (34%) patients had a diagnosis of MCL with an associated hematologic neoplasm (MCL-AHN). Chronic MCL (lack of C-findings) comprised 14% of patients, and only 4.5% had "leukemic MCL" (≥10% circulating MCs). KIT D816V was found in 62/85 (73%) evaluable patients; 9 (11%) individuals exhibited alternative KIT mutations, and no KIT variants were detected in 14 (17%) subjects. Ten evaluable patients (17%) had an abnormal karyotype and the poor-risk SRSF2, ASXL1, and RUNX1 (S/A/R) mutations were identified in 16/36 (44%) patients who underwent next-generation sequencing. Midostaurin was the most common therapy administered to 65% of patients and 45% as first-line therapy. The median overall survival (OS) was 1.6 years. In multivariate analysis (S/A/R mutations excluded owing to low event rates), a diagnosis of MCL-AHN (hazard ratio [HR], 4.7; 95% confidence interval [CI], 1.7-13.0; P = .001) and abnormal karyotype (HR, 5.6; 95% CI, 1.4-13.3; P = .02) were associated with inferior OS; KIT D816V positivity (HR, 0.33; 95% CI, 0.11-0.98; P = .04) and midostaurin treatment (HR, 0.32; 95% CI, 0.08-0.72; P = .008) were associated with superior OS. These data provide the most comprehensive snapshot of the clinicopathologic, molecular, and treatment landscape of MCL to date, and should help further inform subtyping and prognostication of MCL.
肥大细胞白血病(MCL)是一种罕见的系统性肥大细胞增多症亚型,定义为骨髓抽吸物中≥20%的肥大细胞(MC)。我们评估了来自欧洲肥大细胞增多症网络注册中心的 92 名 MCL 患者。31 名(34%)患者患有伴血液系统恶性肿瘤的 MCL(MCL-AHN)。慢性 MCL(无 C 发现)占患者的 14%,仅有 4.5%的患者患有“白血病性 MCL”(≥10%循环 MC)。在可评估的 85 名患者中的 62 名(73%)发现了 KIT D816V;9 名(11%)个体表现出其他 KIT 突变,而 14 名(17%)患者未检测到 KIT 变体。10 名可评估患者(17%)存在异常核型,在接受下一代测序的 36 名患者中发现了 16 名(44%)不良风险的 SRSF2、ASXL1 和 RUNX1(S/A/R)突变。米哚妥林是最常使用的治疗方法,65%的患者接受了该治疗,45%的患者作为一线治疗。中位总生存期(OS)为 1.6 年。在多变量分析中(由于事件发生率低,排除了 S/A/R 突变),MCL-AHN 诊断(危险比[HR],4.7;95%置信区间[CI],1.7-13.0;P =.001)和异常核型(HR,5.6;95%CI,1.4-13.3;P =.02)与较差的 OS 相关;KIT D816V 阳性(HR,0.33;95%CI,0.11-0.98;P =.04)和米哚妥林治疗(HR,0.32;95%CI,0.08-0.72;P =.008)与较好的 OS 相关。这些数据提供了迄今为止对 MCL 的临床病理、分子和治疗情况最全面的快照,应该有助于进一步对 MCL 进行亚型分类和预后判断。