Department of Emergency and Critical Care Medicine, Keio University School of Medicine, Tokyo, Japan.
Department of Emergency and Critical Care Medicine, Tokyo Saiseikai Central Hospital, Tokyo, Japan.
Nephron. 2023;147(3-4):170-176. doi: 10.1159/000526268. Epub 2022 Sep 12.
Post-contrast acute kidney injury (PC-AKI) is a major complication of contrast media usage; risks for PC-AKI are generally evaluated before computed tomography (CT) with contrast at the emergency department (ED). Although persistent hypotension (systolic blood pressure [sBP] <80 mm Hg for 1 h) is associated with increased PC-AKI incidence, it remains unclear whether transient hypotension that is haemodynamically stabilized before CT is a risk of PC-AKI. We hypothesized that hypotension on ED arrival would be associated with higher PC-AKI incidence even if CT with contrast was performed after patients are appropriately resuscitated.
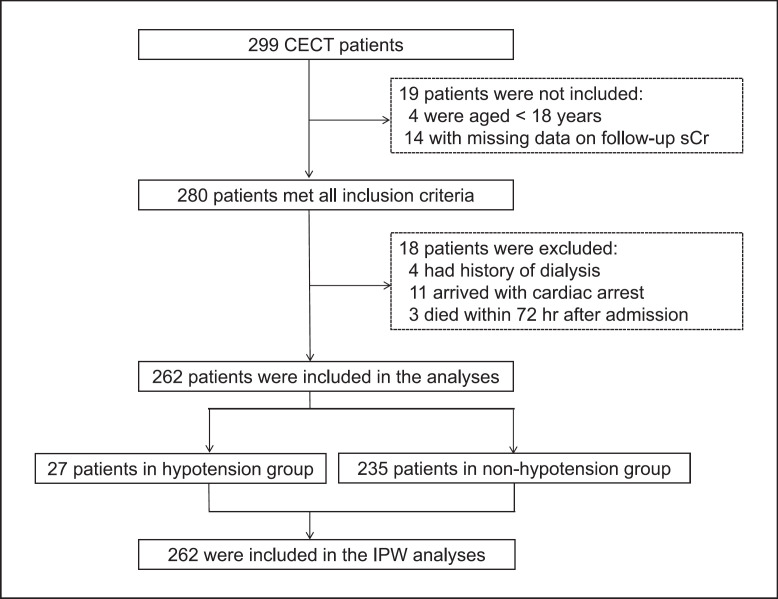
This multicentre retrospective observational study was conducted at three tertiary care centres during 2013-2014. We identified 280 patients who underwent CT with contrast at the ED. Patients were classified into two groups based on sBP on arrival (<80 vs. ≥80 mm Hg); hypotension was considered as transient because CT with contrast has always been performed after patients were stabilized at participating hospitals. PC-AKI incidence was compared between the groups; inverse probability weighting (IPW) was conducted to adjust background characteristics.
Eighteen patients were excluded due to chronic haemodialysis, cardiac arrest on arrival, or death within 72 h; 262 were eligible for this study. PC-AKI incidence was higher in the transient hypotension group than the normotension group {7/27 (28.6%) vs. 24/235 (10.2%), odds ratio (OR) 3.08 (95% confidence interval [CI] 1.18-8.03), p = 0.026}, which was confirmed by IPW (OR 3.25 [95% CI 1.99-5.29], p < 0.001).
Transient hypotension at the ED was associated with PC-AKI development.
造影剂后急性肾损伤(PC-AKI)是造影剂使用的主要并发症;在急诊科(ED)进行 CT 增强检查前,通常会评估 PC-AKI 的风险。虽然持续低血压(收缩压 [sBP]<80mmHg 持续 1 小时)与 PC-AKI 发生率增加相关,但在 CT 增强检查前血流动力学稳定的短暂性低血压是否为 PC-AKI 的风险尚不清楚。我们假设 ED 就诊时的低血压即使在适当复苏后进行 CT 增强检查也会导致更高的 PC-AKI 发生率。
这项多中心回顾性观察性研究于 2013-2014 年在三个三级护理中心进行。我们确定了 280 名在 ED 接受 CT 增强检查的患者。根据到达时的 sBP(<80 与≥80mmHg)将患者分为两组;由于 CT 增强检查总是在患者在参与医院稳定后进行,因此将低血压定义为短暂性低血压。比较两组之间的 PC-AKI 发生率;采用逆概率加权(IPW)调整背景特征。
18 名患者因慢性血液透析、到达时心脏骤停或 72 小时内死亡而被排除在外;262 名患者符合本研究条件。短暂性低血压组的 PC-AKI 发生率高于正常血压组{7/27(28.6%)与 24/235(10.2%),比值比(OR)3.08(95%置信区间 [CI] 1.18-8.03),p=0.026},这一结果通过 IPW 得到了确认(OR 3.25 [95% CI 1.99-5.29],p<0.001)。
ED 短暂性低血压与 PC-AKI 发展相关。