Metabolism, Nutrition, and Atherosclerosis Laboratory, Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Cardiopulmonary Laboratory, Department of Clinical and Experimental Medicine, University of Pisa, Pisa, Italy.
Cardiovasc Diabetol. 2022 Sep 12;21(1):181. doi: 10.1186/s12933-022-01618-1.
The mechanism through which sodium-glucose cotransporter 2 inhibitors (SGLT2i) prevent the incidence of heart failure and/or affect cardiac structure and function remains unclear.
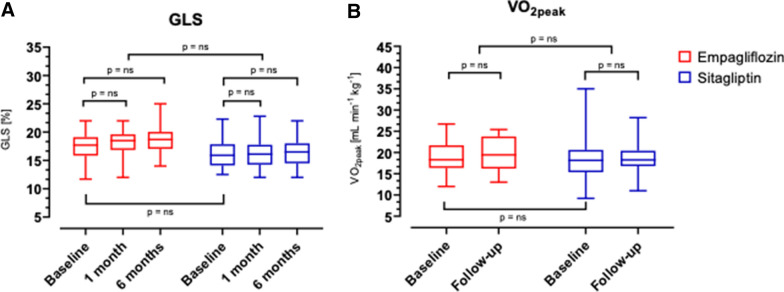
The EMPA-HEART trial is aimed at verifying whether empagliflozin improves myocardial contractility (left ventricle global longitudinal strain, LV-GLS) and/or cardiopulmonary fitness (peak oxygen uptake, VO2peak) in subjects with type 2 diabetes (T2D) without heart disease. Patients with T2D, normal LV systolic function (2D-Echo EF > 50%), and no heart disease were randomized to either empagliflozin 10 mg or sitagliptin 100 mg for 6 months and underwent repeated cardiopulmonary exercise tests with echocardiography and determination of plasma biomarkers.
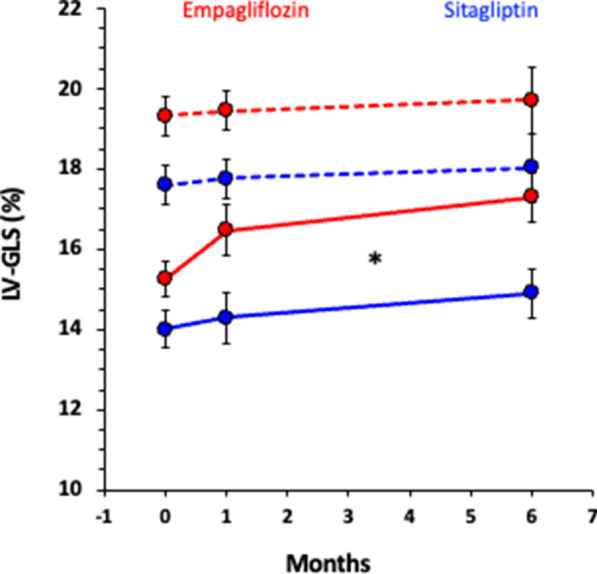
Forty-four patients completed the study, 22 per arm. Despite comparable glycaemic control, modest reductions in body weight (- 1.6; [- 2.7/- 0.5] kg, p = 0.03) and plasma uric acid (- 1.5; [- 2.3/- 0.6], p = 0.002), as well as an increase in haemoglobin (+ 0.7; [+ 0.2/+ 1.1] g/dL, p = 0.0003) were evident with empagliflozin. No difference was detectable in either LV-GLS at 1 month (empagliflozin vs sitagliptin: + 0.44; [- 0.10/+ 0.98]%, p = 0.11) and 6 months of therapy (+ 0.53; [- 0.56/+ 1.62]%), or in VO (+ 0.43; [- 1.4/+ 2.3] mL/min/kg, p = 0.65). With empagliflozin, the subgroup with baseline LV-GLS below the median experienced a greater increase (time*drug p < 0.05) in LV-GLS at 1 month (+ 1.22; [+ 0.31/+ 2.13]%) and 6 months (+ 2.05; [+ 1.14/+ 2.96]%), while sitagliptin induced a modest improvement in LV-GLS only at 6 months (+ 0.92; [+ 0.21/+ 0.62]%).
Empagliflozin has neutral impact on both LV-GLS and exercise tolerance in subjects with T2D and normal left ventricular function. However, in patients with subclinical dysfunction (LV-GLS < 16.5%) it produces a rapid and sustained amelioration of LV contractility. Trial registration EUDRACT Code 2016-002225-10.
钠-葡萄糖协同转运蛋白 2 抑制剂(SGLT2i)预防心力衰竭发生和/或影响心脏结构和功能的机制仍不清楚。
EMPA-HEART 试验旨在验证恩格列净是否能改善 2 型糖尿病(T2D)患者无心脏病的心肌收缩力(左心室整体纵向应变,LV-GLS)和/或心肺功能(峰值摄氧量,VO2peak)。T2D 患者、左心室收缩功能正常(2D-Echo EF>50%)且无心脏病,被随机分为恩格列净 10mg 或西格列汀 100mg 组,治疗 6 个月,并进行重复心肺运动试验,同时行超声心动图检查和测定血浆生物标志物。
44 例患者完成了研究,每组 22 例。尽管血糖控制相当,但恩格列净组体重明显减轻(-1.6;[-2.7/-0.5]kg,p=0.03),血浆尿酸降低(-1.5;[-2.3/-0.6],p=0.002),血红蛋白升高(+0.7;[+0.2/+1.1]g/dL,p=0.0003)。恩格列净治疗 1 个月(恩格列净与西格列汀:+0.44;[-0.10/+0.98]%,p=0.11)和 6 个月时,LV-GLS 均无差异(+0.53;[-0.56/+1.62]%),VO 也无差异(+0.43;[-1.4/+2.3]mL/min/kg,p=0.65)。在恩格列净组中,基线 LV-GLS 低于中位数的亚组在 1 个月(+1.22;[+0.31/+2.13]%)和 6 个月时(+2.05;[+1.14/+2.96]%)的 LV-GLS 增加更明显(时间*药物 p<0.05),而西格列汀仅在 6 个月时改善 LV-GLS(+0.92;[+0.21/+0.62]%)。
恩格列净对 T2D 患者左心室功能正常的患者的 LV-GLS 和运动耐量无影响。然而,在有亚临床功能障碍(LV-GLS<16.5%)的患者中,它能迅速且持续改善左心室收缩功能。
试验注册 EUDRACT 编号 2016-002225-10。