Chartash David, Rosenman Marc, Wang Karen, Chen Elizabeth
School of Medicine, University College Dublin - National University of Ireland, Dublin, Ireland.
Center for Medical Informatics, Yale University School of Medicine, New Haven, CT, United States.
JMIR Med Educ. 2022 Sep 13;8(3):e39794. doi: 10.2196/39794.
With the advent of competency-based medical education, as well as Canadian efforts to include clinical informatics within undergraduate medical education, competency frameworks in the United States have not emphasized the skills associated with clinical informatics pertinent to the broader practice of medicine.
By examining the competency frameworks with which undergraduate medical education in clinical informatics has been developed in Canada and the United States, we hypothesized that there is a gap: the lack of a unified competency set and frame for clinical informatics education across North America.
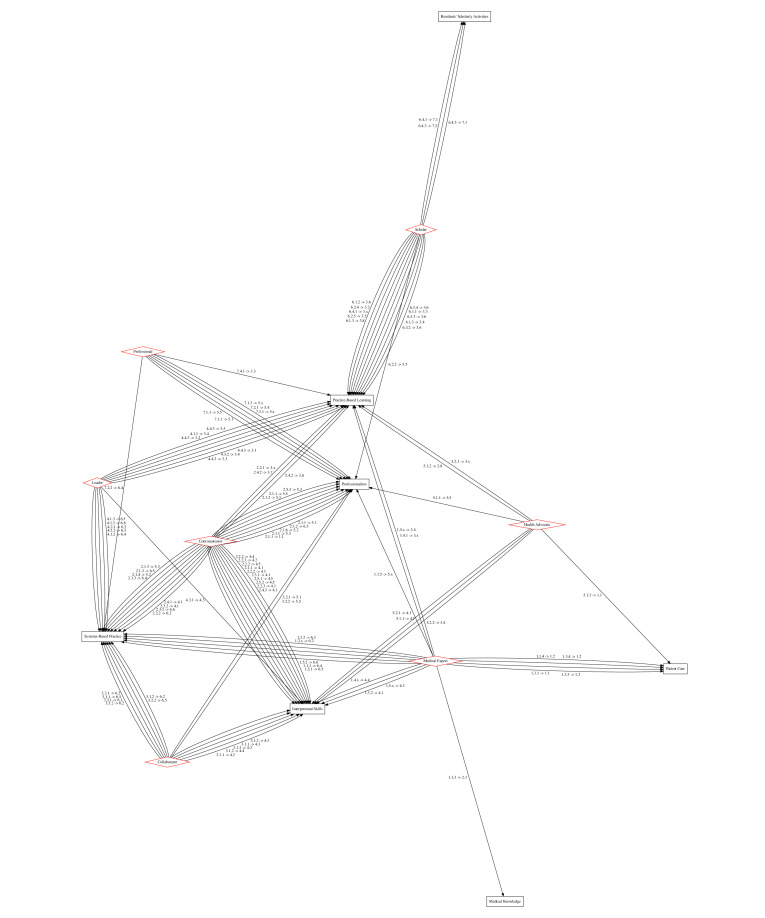
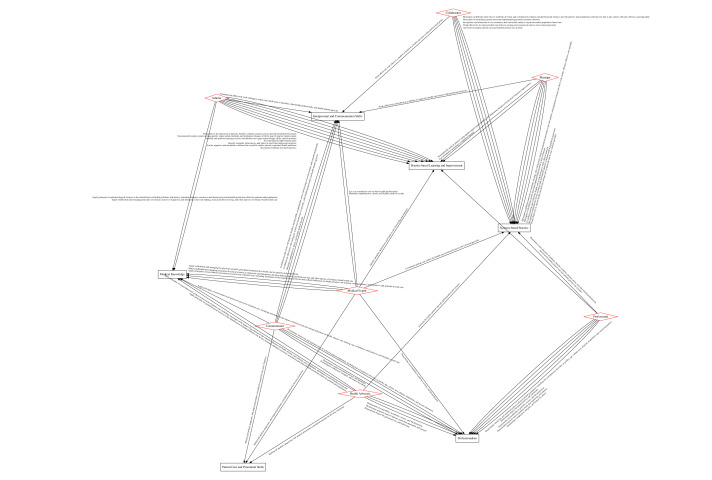
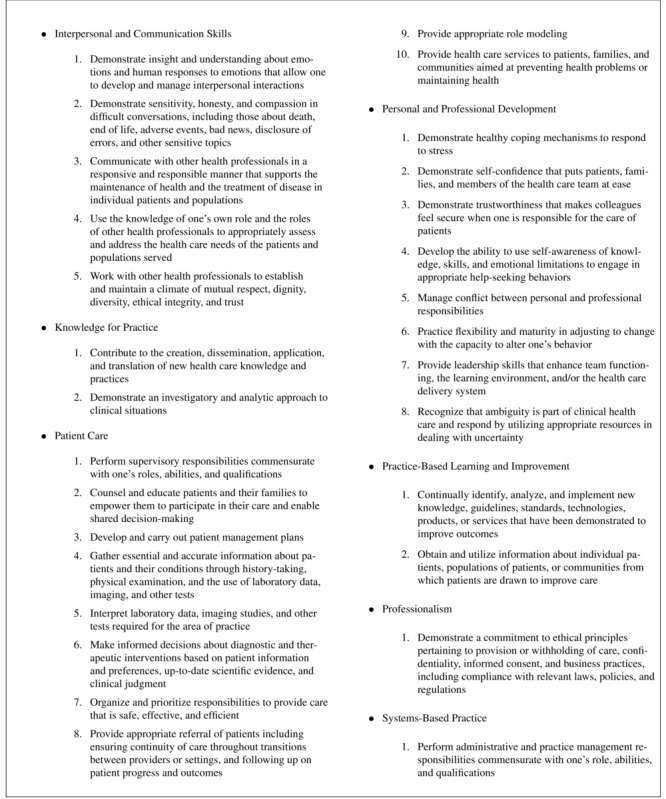
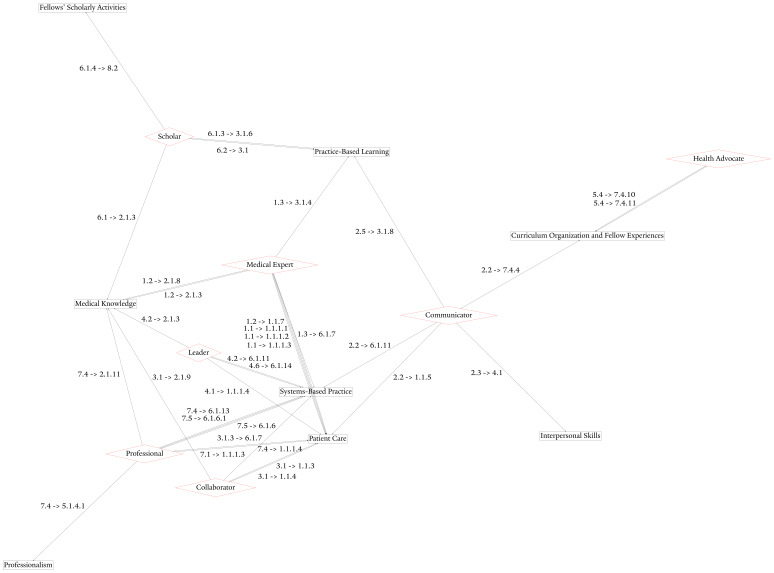
We performed directional competency mapping between Canadian and American graduate clinical informatics competencies and general graduate medical education competencies. Directional competency mapping was performed between Canadian roles and American common program requirements using keyword matching at the subcompetency and enabling competency levels. In addition, for general graduate medical education competencies, the Physician Competency Reference Set developed for the Liaison Committee on Medical Education was used as a direct means of computing the ontological overlap between competency frameworks.
Upon mapping Canadian roles to American competencies via both undergraduate and graduate medical education competency frameworks, the difference in focus between the 2 countries can be thematically described as a difference between the concepts of clinical and management reasoning.
We suggest that the development or deployment of informatics competencies in undergraduate medical education should focus on 3 items: the teaching of diagnostic reasoning, such that the information tasks that comprise both clinical and management reasoning can be discussed; precision medical education, where informatics can provide for more fine-grained evaluation; and assessment methods to support traditional pedagogical efforts (both at the bedside and beyond). Assessment using cases or structured assessments (eg, Objective Structured Clinical Examinations) would help students draw parallels between clinical informatics and fundamental clinical subjects and would better emphasize the cognitive techniques taught through informatics.
随着基于能力的医学教育的出现,以及加拿大将临床信息学纳入本科医学教育的努力,美国的能力框架并未强调与更广泛医学实践相关的临床信息学技能。
通过研究加拿大和美国本科临床信息学医学教育所采用的能力框架,我们推测存在一个差距:北美缺乏统一的临床信息学教育能力集和框架。
我们对加拿大和美国研究生临床信息学能力与普通研究生医学教育能力进行了定向能力映射。使用子能力和促成能力层面的关键词匹配,在加拿大的角色和美国的共同项目要求之间进行定向能力映射。此外,对于普通研究生医学教育能力,为医学教育联络委员会制定的《医师能力参考集》被用作计算能力框架之间本体重叠的直接手段。
通过本科和研究生医学教育能力框架将加拿大的角色映射到美国的能力后,两国之间重点的差异可以从主题上描述为临床推理和管理推理概念之间的差异。
我们建议本科医学教育中信息学能力的开发或部署应关注三个方面:诊断推理教学,以便能够讨论构成临床推理和管理推理的信息任务;精准医学教育,信息学可在其中提供更精细的评估;以及支持传统教学工作(包括床边教学和其他教学)的评估方法。使用案例或结构化评估(如客观结构化临床考试)进行评估将有助于学生在临床信息学和基础临床学科之间建立联系,并能更好地强调通过信息学教授的认知技巧。