Department of Hematology, First Affiliated Hospital of Nanjing Medical University, Jiangsu Province Hospital, Collaborative Innovation Center for Cancer Personalized Medicine, Nanjing, China.
State Key Laboratory of Experimental Hematology, National Clinical Research Center for Blood Diseases, Haihe Laboratory of Cell Ecosystem, Institute of Hematology & Blood Diseases Hospital, Chinese Academy of Medical Sciences & Peking Union Medical College, Tianjin, China.
J Immunother Cancer. 2022 Sep;10(9). doi: 10.1136/jitc-2022-005145.
Anti-B-cell maturation antigen (BCMA) chimeric antigen receptor T-cell (CAR T) therapy showed remarkable efficacy in patients with relapsed or refractory multiple myeloma (RRMM). This phase 1 dose-escalation and expansion study developed C-CAR088, a novel second-generation humanized anti-BCMA CAR T-cell therapy, and assessed the safety and efficacy of three dosages of C-CAR088 in patients with RRMM.
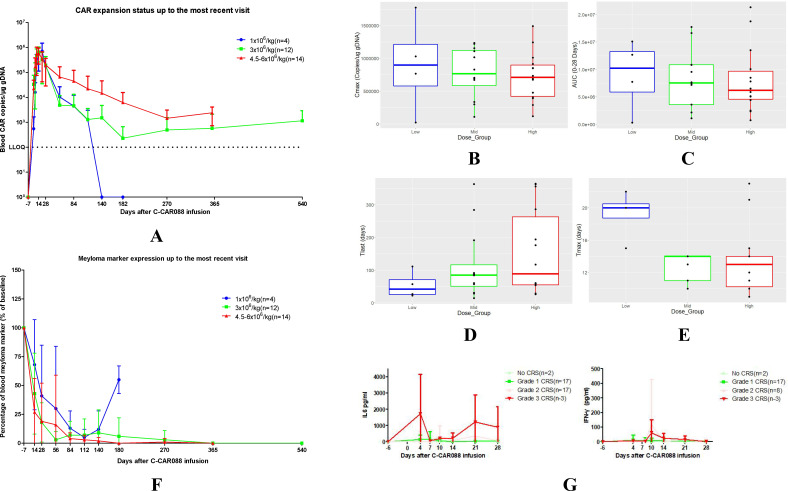
Patients received lymphodepletion with three doses of cyclophosphamide (300 mg/m) and three doses of fludarabine (30 mg/m) on days -5, -4, and -3, followed by an infusion of C-CAR088 on day 0. Doses of 1.0×10, 3.0×10, and 6.0×10 CAR T cells/kg (±20%) were tested in the dose-escalation cohorts and expansion cohorts. The primary endpoint was treatment safety, including the rate of treatment-emergent adverse events after cell infusion. Secondary endpoints were the overall response rate and progression-free survival. The exploratory endpoints were the quantification of C-CAR088 CAR T cells, selection of cytokines and chemokines in blood, and measurement of tumor BCMA expression.
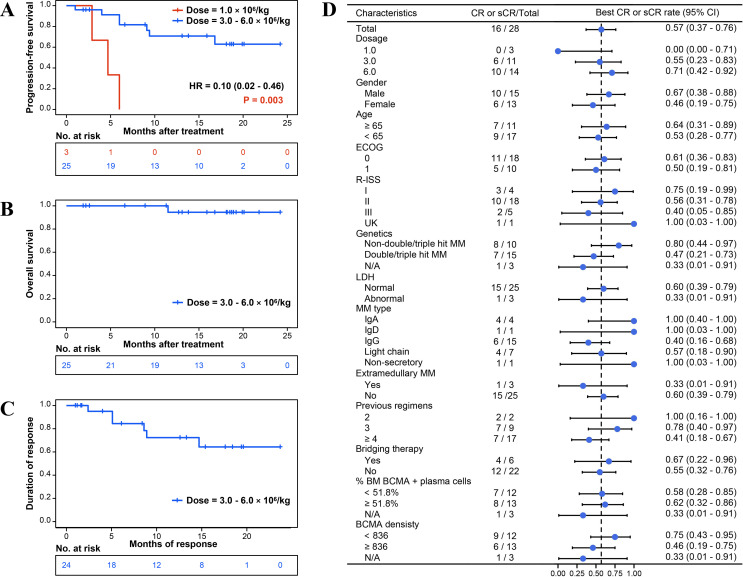
As of July 2, 2021, 31 patients had been infused with C-CAR088. Any grade cytokine release syndrome (CRS) occurred in 29 patients (93.5%), and grade 3 CRS occurred in 3 patients (9.7%). One patient from the high-dose group (4.5-6.0×10 CAR T cells/kg) developed grade 1 neurotoxicity. No dose-limiting toxicities were observed in any dose group, and all adverse events were reversible after proper management. The overall response, stringent complete response, complete response (CR), and very good partial response rates were 96.4%, 46.4%, 10.7%, and 32.1%, respectively. The CR rate in the medium-dose (3.0×10 CAR T cells/kg) and high-dose (4.5-6.0×10 CAR T cells/kg) groups was 54.5% and 71.4%, respectively. In the CR group, 15 (93.7%) patients achieved minimal residual disease (MRD) negativity (test sensitivity >1/10). All seven patients with double-hit or triple-hit multiple myeloma achieved MRD-negative CR.
The present study demonstrated that C-CAR088 had a good safety profile and high antitumor activity in patients with RRMM, constituting a promising treatment option for RRMM.
NCT03815383, NCT03751293, NCT04295018, and NCT04322292.
抗 B 细胞成熟抗原(BCMA)嵌合抗原受体 T 细胞(CAR T)疗法在复发或难治性多发性骨髓瘤(RRMM)患者中显示出显著疗效。这项 1 期剂量递增和扩展研究开发了 C-CAR088,这是一种新型第二代人源化抗 BCMA CAR T 细胞疗法,并评估了三种剂量的 C-CAR088 在 RRMM 患者中的安全性和疗效。
患者在第-5、-4 和-3 天接受环磷酰胺(300mg/m)和氟达拉滨(30mg/m)三剂淋巴细胞耗竭治疗,随后在第 0 天输注 C-CAR088。在剂量递增队列和扩展队列中测试了 1.0×10、3.0×10 和 6.0×10⁻CAR T 细胞/kg(±20%)的剂量。主要终点是治疗后细胞输注后的治疗出现的不良事件发生率,包括治疗相关不良事件的发生率。次要终点是总缓解率和无进展生存期。探索终点是 C-CAR088 CAR T 细胞的定量、血液中细胞因子和趋化因子的选择以及肿瘤 BCMA 表达的测量。
截至 2021 年 7 月 2 日,已有 31 名患者接受了 C-CAR088 输注。29 名患者(93.5%)出现任何级别细胞因子释放综合征(CRS),3 名患者(9.7%)出现 3 级 CRS。高剂量组(4.5-6.0×10⁻CAR T 细胞/kg)的 1 名患者出现 1 级神经毒性。任何剂量组均未观察到剂量限制毒性,所有不良事件经适当治疗后均可逆转。总缓解率、严格完全缓解率、完全缓解率(CR)和非常好的部分缓解率分别为 96.4%、46.4%、10.7%和 32.1%。中剂量(3.0×10⁻CAR T 细胞/kg)和高剂量(4.5-6.0×10⁻CAR T 细胞/kg)组的 CR 率分别为 54.5%和 71.4%。在 CR 组中,15 名(93.7%)患者达到最小残留疾病(MRD)阴性(检测灵敏度>1/10)。所有 7 名患有双打击或三打击多发性骨髓瘤的患者均达到 MRD 阴性的 CR。
本研究表明 C-CAR088 在 RRMM 患者中具有良好的安全性和高抗肿瘤活性,是 RRMM 的一种有前途的治疗选择。
NCT03815383、NCT03751293、NCT04295018 和 NCT04322292。