Cardiovascular Research Institute, University of California San Francisco, 503 Parnassus Ave, HSE 760, San Francisco, CA, 94143, USA.
Division of Critical Care, Departments of Medicine and Microbiology and Immunology, Western University, London, ON, Canada.
Crit Care. 2022 Sep 14;26(1):278. doi: 10.1186/s13054-022-04153-3.
Studies quantifying SARS-CoV-2 have focused on upper respiratory tract or plasma viral RNA with inconsistent association with clinical outcomes. The association between plasma viral antigen levels and clinical outcomes has not been previously studied. Our aim was to investigate the relationship between plasma SARS-CoV-2 nucleocapsid antigen (N-antigen) concentration and both markers of host response and clinical outcomes.
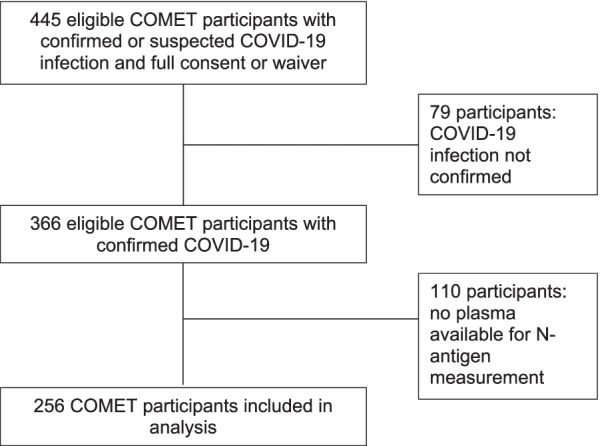
SARS-CoV-2 N-antigen concentrations were measured in the first study plasma sample (D0), collected within 72 h of hospital admission, from 256 subjects admitted between March 2020 and August 2021 in a prospective observational cohort of hospitalized patients with COVID-19. The rank correlations between plasma N-antigen and plasma biomarkers of tissue damage, coagulation, and inflammation were assessed. Multiple ordinal regression was used to test the association between enrollment N-antigen plasma concentration and the primary outcome of clinical deterioration at one week as measured by a modified World Health Organization (WHO) ordinal scale. Multiple logistic regression was used to test the association between enrollment plasma N-antigen concentration and the secondary outcomes of ICU admission, mechanical ventilation at 28 days, and death at 28 days. The prognostic discrimination of an externally derived "high antigen" cutoff of N-antigen ≥ 1000 pg/mL was also tested.
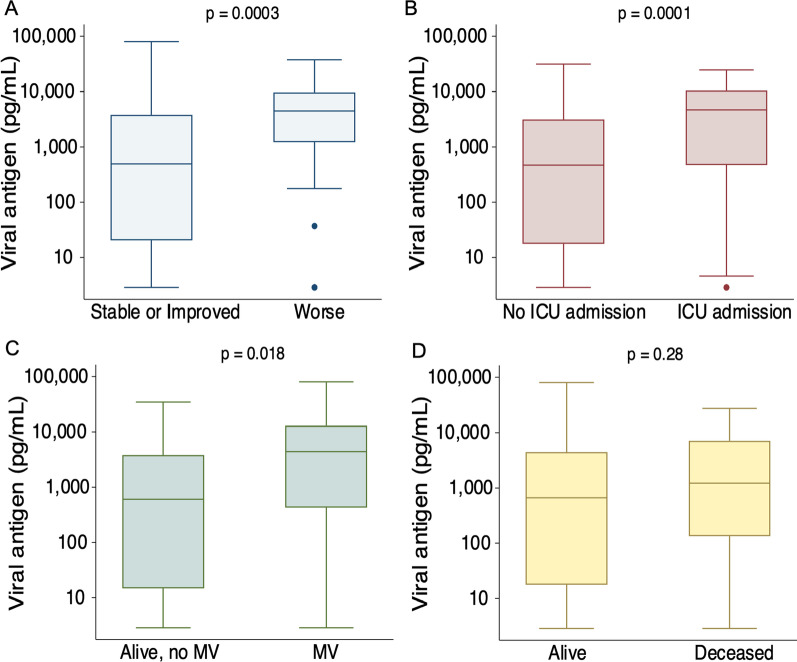
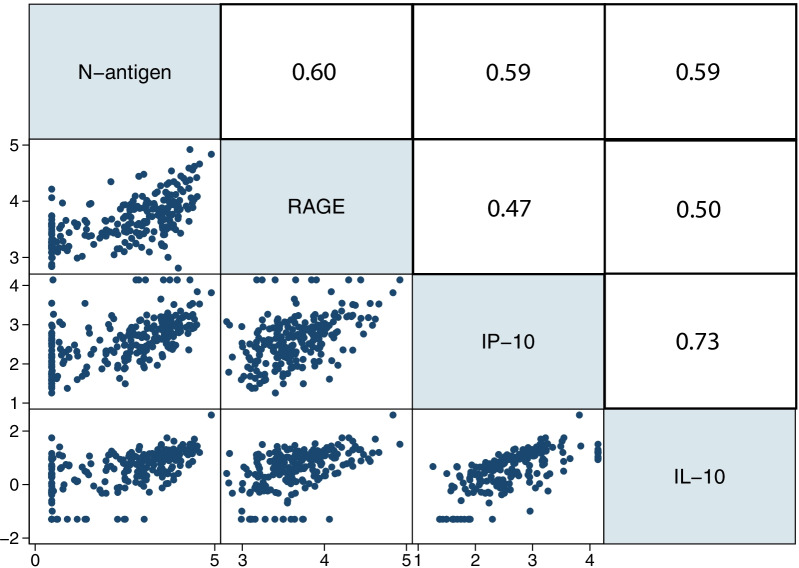
N-antigen on D0 was detectable in 84% of study participants. Plasma N-antigen levels significantly correlated with RAGE (r = 0.61), IL-10 (r = 0.59), and IP-10 (r = 0.59, adjusted p = 0.01 for all correlations). For the primary outcome of clinical status at one week, each 500 pg/mL increase in plasma N-antigen level was associated with an adjusted OR of 1.05 (95% CI 1.03-1.08) for worse WHO ordinal status. D0 plasma N-antigen ≥ 1000 pg/mL was 77% sensitive and 59% specific (AUROC 0.68) with a positive predictive value of 23% and a negative predictive value of 93% for a worse WHO ordinal scale at day 7 compared to baseline. D0 N-antigen concentration was independently associated with ICU admission and 28-day mechanical ventilation, but not with death at 28 days.
Plasma N-antigen levels are readily measured and provide important insight into the pathogenesis and prognosis of COVID-19. The measurement of N-antigen levels early in-hospital course may improve risk stratification, especially for identifying patients who are unlikely to progress to severe disease.
定量检测 SARS-CoV-2 的研究主要集中在上呼吸道或血浆中的病毒 RNA,其与临床结局的相关性并不一致。血浆病毒抗原水平与临床结局之间的关系尚未被研究过。我们的目的是研究血浆 SARS-CoV-2 核衣壳抗原(N-抗原)浓度与宿主反应标志物和临床结局之间的关系。
我们在 2020 年 3 月至 2021 年 8 月期间,前瞻性观察性地纳入了 256 例因 COVID-19 住院的患者,采集他们入院后 72 小时内的首份研究血浆样本(D0),并测量了其中的 SARS-CoV-2 N-抗原浓度。评估了血浆 N-抗原与组织损伤、凝血和炎症的血浆生物标志物之间的秩相关关系。采用多变量有序回归检验入院时 N-抗原血浆浓度与一周时临床恶化的主要结局(根据世界卫生组织(WHO)的改良 ordinal 量表进行测量)之间的关联。采用多变量逻辑回归检验入院时 N-抗原血浆浓度与次要结局(28 天内 ICU 入院、28 天内机械通气和 28 天内死亡)之间的关联。还检验了外部衍生的 N-抗原 cutoff 值(N-抗原≥1000pg/ml)的预后预测能力。
研究参与者中有 84%的人在 D0 可检测到 N-抗原。血浆 N-抗原水平与 RAGE(r=0.61)、IL-10(r=0.59)和 IP-10(r=0.59,所有相关性的调整 p=0.01)显著相关。对于一周时的临床状态这一主要结局,血浆 N-抗原水平每增加 500pg/ml,调整后的 OR 为 1.05(95%CI 1.03-1.08),WHO ordinal 状态更差。D0 时血浆 N-抗原≥1000pg/ml 的敏感性为 77%,特异性为 59%(AUROC 0.68),预测 7 天时 WHO ordinal 量表恶化的阳性预测值为 23%,阴性预测值为 93%。与基线相比,D0 时 N-抗原浓度与 ICU 入院和 28 天机械通气独立相关,但与 28 天死亡无关。
血浆 N-抗原水平容易测量,为 COVID-19 的发病机制和预后提供了重要的见解。在住院早期检测 N-抗原水平可能会改善风险分层,尤其是可以识别不太可能进展为严重疾病的患者。