Meso Scale Diagnostics, LLC, Rockville, Maryland, USA.
Department of Anesthesiology, Critical Care and Pain Medicine, Boston Children's Hospital, and Department of Anesthesia, Harvard Medical School, Boston, Massachusetts, USA.
Clin Infect Dis. 2022 Oct 12;75(8):1351-1358. doi: 10.1093/cid/ciac160.
Detection of severe acute respiratory syndrome coronavirus 2 (SARS-CoV-2) antigens in blood has high sensitivity in adults with acute coronavirus disease 2019 (COVID-19), but sensitivity in pediatric patients is unclear. Recent data suggest that persistent SARS-CoV-2 spike antigenemia may contribute to multisystem inflammatory syndrome in children (MIS-C). We quantified SARS-CoV-2 nucleocapsid (N) and spike (S) antigens in blood of pediatric patients with either acute COVID-19 or MIS-C using ultrasensitive immunoassays (Meso Scale Discovery).
Plasma was collected from inpatients (<21 years) enrolled across 15 hospitals in 15 US states. Acute COVID-19 patients (n = 36) had a range of disease severity and positive nasopharyngeal SARS-CoV-2 RT-PCR within 24 hours of blood collection. Patients with MIS-C (n = 53) met CDC criteria and tested positive for SARS-CoV-2 (RT-PCR or serology). Controls were patients pre-COVID-19 (n = 67) or within 24 hours of negative RT-PCR (n = 43).
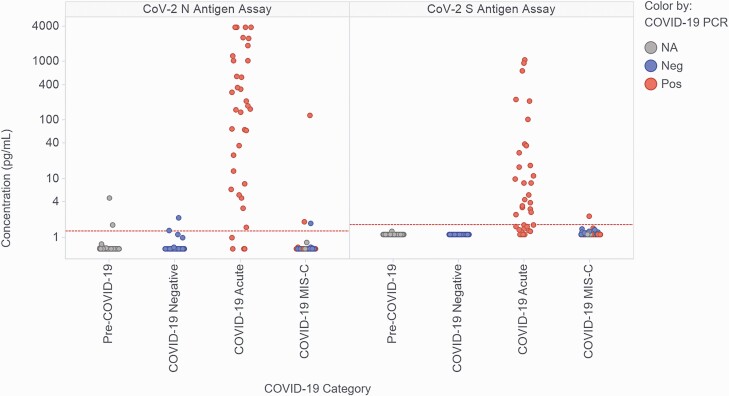
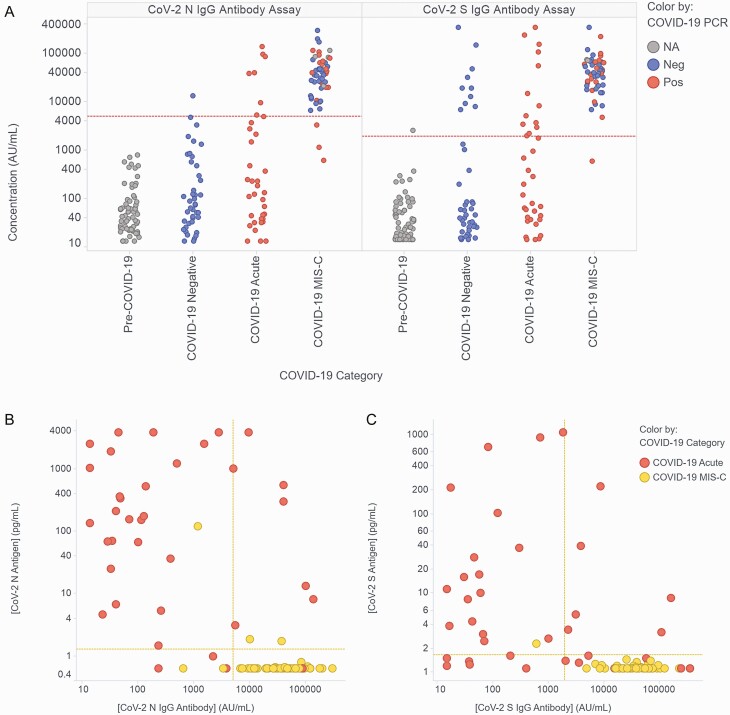
Specificities of N and S assays were 95-97% and 100%, respectively. In acute COVID-19 patients, N/S plasma assays had 89%/64% sensitivity; sensitivities in patients with concurrent nasopharyngeal swab cycle threshold (Ct) ≤35 were 93%/63%. Antigen concentrations ranged from 1.28-3844 pg/mL (N) and 1.65-1071 pg/mL (S) and correlated with disease severity. In MIS-C, antigens were detected in 3/53 (5.7%) samples (3 N-positive: 1.7, 1.9, 121.1 pg/mL; 1 S-positive: 2.3 pg/mL); the patient with highest N had positive nasopharyngeal RT-PCR (Ct 22.3) concurrent with blood draw.
Ultrasensitive blood SARS-CoV-2 antigen measurement has high diagnostic yield in children with acute COVID-19. Antigens were undetectable in most MIS-C patients, suggesting that persistent antigenemia is not a common contributor to MIS-C pathogenesis.
在患有急性 2019 年冠状病毒病(COVID-19)的成年人中,检测严重急性呼吸综合征冠状病毒 2(SARS-CoV-2)抗原具有很高的灵敏度,但在儿科患者中的灵敏度尚不清楚。最近的数据表明,持续的 SARS-CoV-2 刺突抗原血症可能导致儿童多系统炎症综合征(MIS-C)。我们使用超敏免疫测定法(Meso Scale Discovery)定量检测了患有急性 COVID-19 或 MIS-C 的儿科患者血液中的 SARS-CoV-2 核衣壳(N)和刺突(S)抗原。
采集了来自全美 15 个州 15 家医院住院的年龄小于 21 岁的患者的血浆。急性 COVID-19 患者(n=36)疾病严重程度不一,在采血后 24 小时内鼻咽 SARS-CoV-2 RT-PCR 呈阳性。MIS-C 患者(n=53)符合 CDC 标准,并通过 SARS-CoV-2(RT-PCR 或血清学)检测呈阳性。对照组为 COVID-19 前患者(n=67)或 24 小时内 RT-PCR 阴性的患者(n=43)。
N 和 S 检测的特异性分别为 95-97%和 100%。在急性 COVID-19 患者中,N/S 血浆检测的灵敏度分别为 89%/64%;同时鼻咽拭子循环阈值(Ct)≤35 的患者的灵敏度分别为 93%/63%。抗原浓度范围为 1.28-3844 pg/mL(N)和 1.65-1071 pg/mL(S),与疾病严重程度相关。在 MIS-C 中,在 53 例患者中的 3 例(5.7%)样本中检测到抗原(3 例 N 阳性:1.7、1.9、121.1 pg/mL;1 例 S 阳性:2.3 pg/mL);N 值最高的患者鼻咽 RT-PCR(Ct 22.3)与血液采集同时呈阳性。
超敏血液 SARS-CoV-2 抗原检测在急性 COVID-19 儿童中具有较高的诊断效能。大多数 MIS-C 患者中无法检测到抗原,表明持续的抗原血症不是 MIS-C 发病机制的常见原因。