Giannarini Gianluca, Rossanese Marta, Macchione Luciano, Mucciardi Giuseppe, Crestani Alessandro, Ficarra Vincenzo
Urology Unit, Santa Maria della Misericordia University Hospital, Udine, Italy.
Urology Section, Gaetano Barresi Department of Human and Paediatric Pathology, University of Messina, Messina, Italy.
Eur Urol Open Sci. 2022 Sep 8;44:162-168. doi: 10.1016/j.euros.2022.08.016. eCollection 2022 Oct.
Acquired bladder diverticula (BD) are a possible complication of bladder outlet obstruction (BOO) due to benign prostate enlargement (BPE). Robot-assisted bladder diverticulectomy (RABD) has been proposed as an alternative to open removal; however, only a few small series have been published.
To describe our surgical technique for RABD and to assess perioperative results and functional outcomes at 6-mo follow-up.
A prospective single-centre, single-surgeon cohort of 16 consecutive men with posterior or posterolateral BD due to BOO/BPE undergoing RABD between May 2017 and December 2021 was analysed.
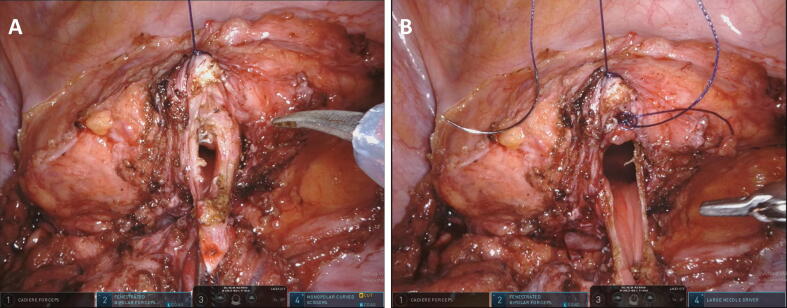
RABD was performed with a four-arm robotic system via a transperitoneal approach. BD were identified intraoperatively via bladder distension with saline solution through an indwelling catheter with or without concomitant illumination using flexible cystoscopy and fluorescence imaging. Extravesical BD dissection and removal were performed.
Operating room time, estimated blood loss, intraoperative and postoperative complications, indwelling catheter time, and timing of associated procedures for BOO/BPE were assessed. The International Prostate Symptom Score (IPSS) and postvoid residual volume (PVR) were compared between baseline and 6 mo after surgery.
Median age and maximum BD diameter were 68 yr (interquartile range [IQR] 54-74) and 69 mm (IQR 51-82), respectively. The median operative time was 126 min (IQR 92-167) and the median estimated blood loss was 20 ml (IQR 15-40). No intraoperative complications were recorded. The urethral catheter was removed on median postoperative day 5 (IQR 5-7). Two men experienced 90-d postoperative complications (persistent urinary infection requiring prolonged antimicrobial therapy). Bipolar transurethral resection of the prostate was performed 3 wk before RABD in seven men and concomitant to RABD in nine men. Median IPSS significantly decreased from 25 (IQR 21-30) to 5 (IQR 5-6), and median PVR from 195 ml (IQR 140-210 ml) to 30 (IQR 28-40) ml (both < 0.001) at 6-mo follow-up in comparison to baseline. A limitation is the rather small cohort with no control group.
RABD is a safe and effective minimally invasive option for treatment of acquired BD in men with BOO/BPE. Validation of our results in larger series with longer follow-up is warranted.
We describe our surgical technique for robot-assisted removal of pouches in the bladder wall (called diverticula) in men with bladder outlet obstruction caused by benign prostate enlargement, and report functional results at 6 months after the operation. This minimally invasive technique was found to be safe and effective.
获得性膀胱憩室(BD)是良性前列腺增生(BPE)导致膀胱出口梗阻(BOO)的一种可能并发症。机器人辅助膀胱憩室切除术(RABD)已被提议作为开放手术切除的替代方法;然而,仅有少数小样本系列报道。
描述我们的RABD手术技术,并评估6个月随访时的围手术期结果和功能结局。
设计、场所和参与者:分析了2017年5月至2021年12月期间16例因BOO/BPE导致后位或后外侧BD的连续男性患者组成的前瞻性单中心、单术者队列,这些患者均接受了RABD。
使用四臂机器人系统经腹腔途径进行RABD。术中通过经留置导尿管向膀胱内注入生理盐水使其扩张,并使用柔性膀胱镜和荧光成像(有或无辅助照明)来识别BD。进行膀胱外BD的分离和切除。
评估手术时间、估计失血量、术中及术后并发症、留置导尿管时间以及BOO/BPE相关手术的时机。比较基线时和术后6个月的国际前列腺症状评分(IPSS)和残余尿量(PVR)。
中位年龄和BD最大直径分别为68岁(四分位间距[IQR]54 - 74)和69 mm(IQR 51 - 82)。中位手术时间为126分钟(IQR 92 - 167),中位估计失血量为20 ml(IQR 15 - 40)。未记录到术中并发症。术后中位第5天(IQR 5 - )拔除尿道导尿管。两名男性出现术后90天并发症(持续性尿路感染,需要延长抗菌治疗)。7名男性在RABD前3周进行了双极经尿道前列腺切除术,9名男性在RABD同时进行了该手术。与基线相比,6个月随访时中位IPSS从25(IQR 21 - 30)显著降至5(IQR 5 - 6),中位PVR从195 ml(IQR 140 - 210 ml)降至30(IQR 28 - 40)ml(两者均<0.001)。局限性在于样本量较小且无对照组。
RABD是治疗因BOO/BPE导致获得性BD男性患者的一种安全有效的微创选择。有必要在更大样本量、更长随访时间的系列研究中验证我们的结果。
我们描述了在良性前列腺增生导致膀胱出口梗阻的男性患者中,机器人辅助切除膀胱壁袋状结构(称为憩室) 的手术技术,并报告了术后6个月的功能结果。发现这种微创技术是安全有效的。