Division of Biomedical Statistics and Informatics, Department of Quantitative Health Sciences Research, Mayo Clinic, Rochester, Minnesota.
Department of Pathology, The University of Chicago., Chicago, Illinois.
Mol Cancer Res. 2022 Dec 2;20(12):1739-1750. doi: 10.1158/1541-7786.MCR-22-0099.
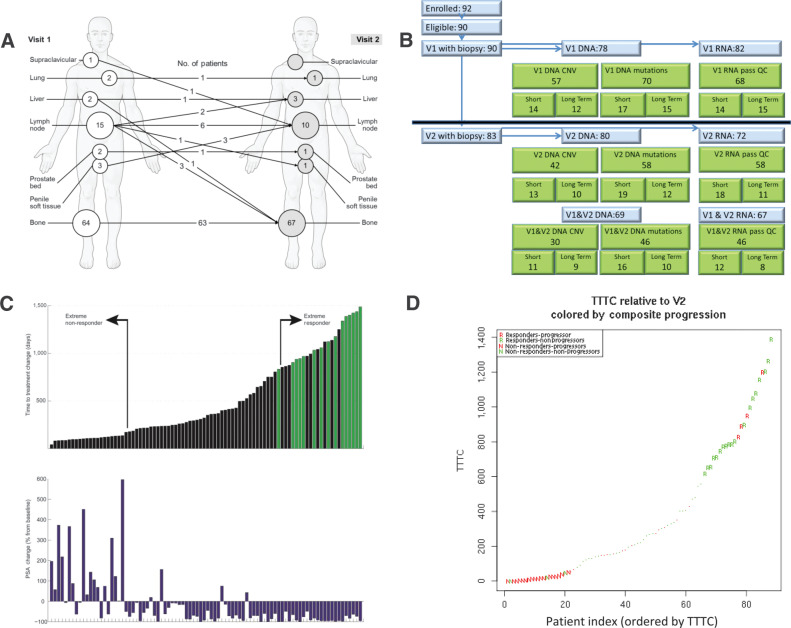
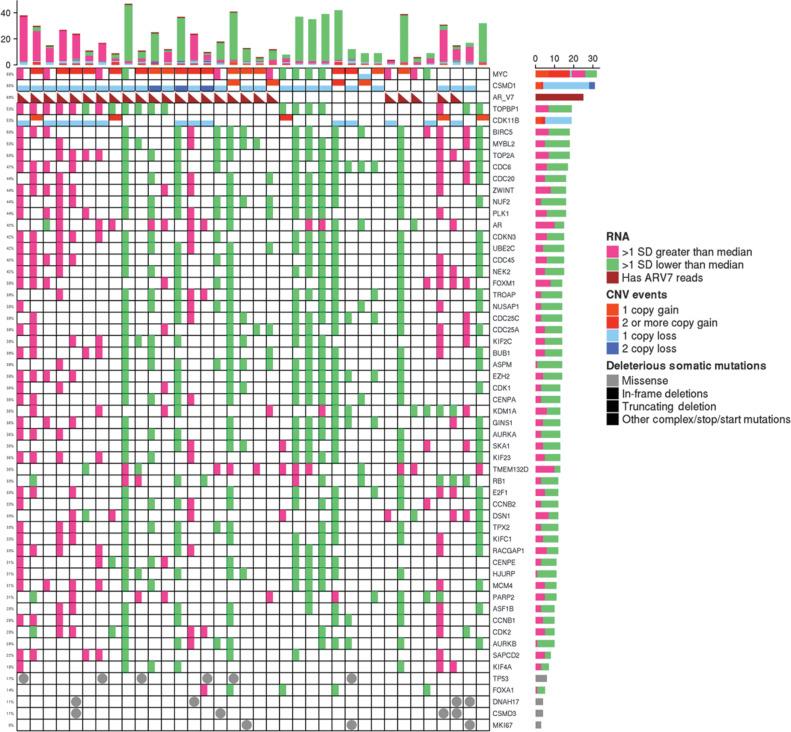
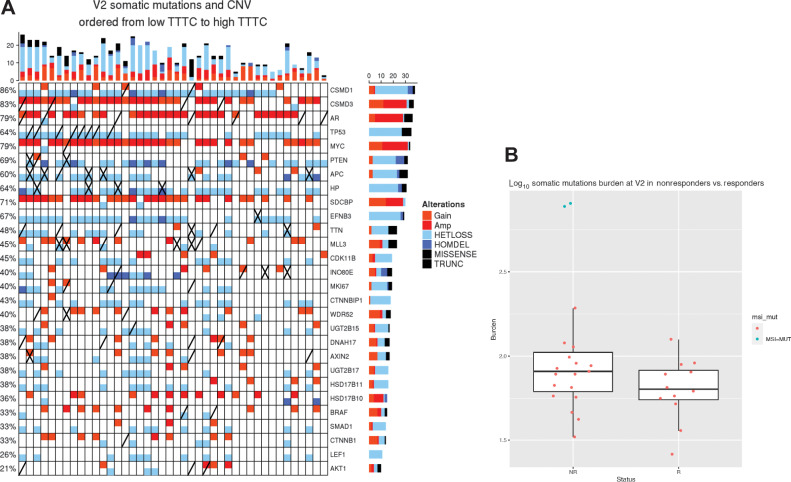
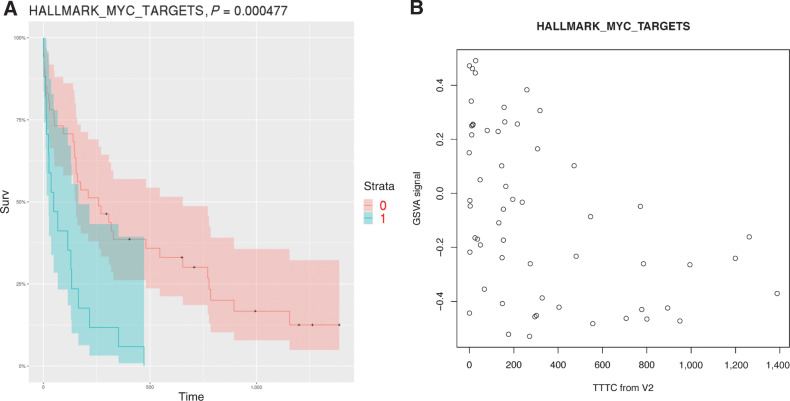
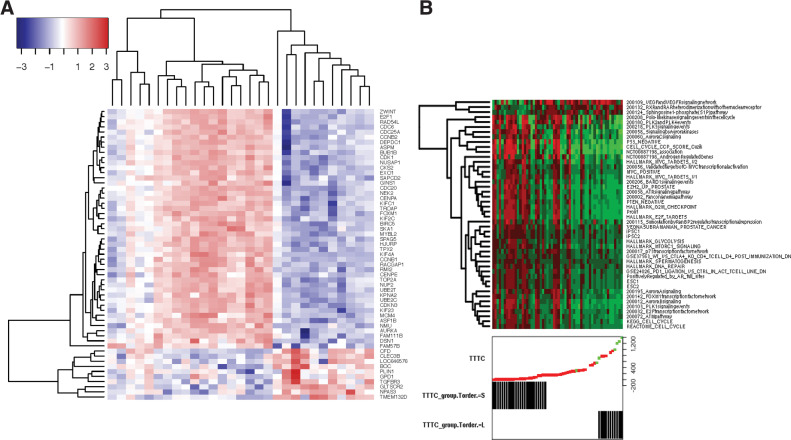
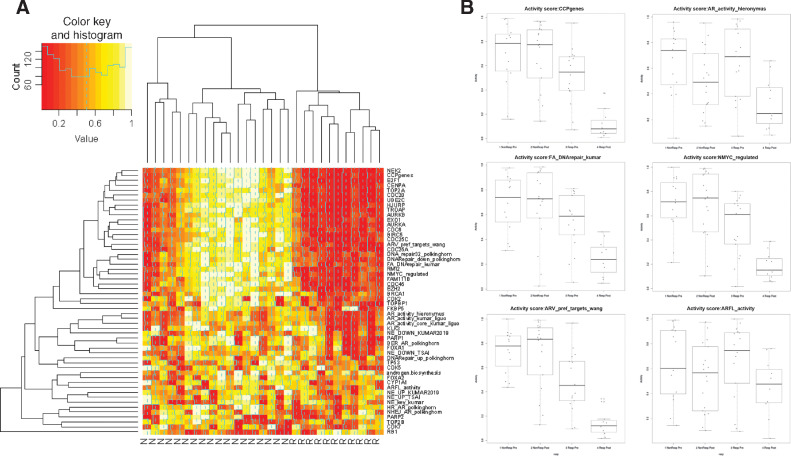
We identified resistance mechanisms to abiraterone acetate/prednisone (AA/P) in patients with metastatic castration-resistant prostate cancer (mCRPC) in the Prostate Cancer Medically Optimized Genome-Enhanced Therapy (PROMOTE) study. We analyzed whole-exome sequencing (WES) and RNA-sequencing data from 83 patients with metastatic biopsies before (V1) and after 12 weeks of AA/P treatment (V2). Resistance was determined by time to treatment change (TTTC). At V2, 18 and 11 of 58 patients had either short-term (median 3.6 months; range 1.4-4.5) or long-term (median 29 months; range 23.5-41.7) responses, respectively. Nonresponders had low expression of TGFBR3 and increased activation of the Wnt pathway, cell cycle, upregulation of AR variants, both pre- and posttreatment, with further deletion of AR inhibitor CDK11B posttreatment. Deletion of androgen processing genes, HSD17B11, CYP19A1 were observed in nonresponders posttreatment. Genes involved in cell cycle, DNA repair, Wnt-signaling, and Aurora kinase pathways were differentially expressed between the responder and non-responder at V2. Activation of Wnt signaling in nonresponder and deactivation of MYC or its target genes in responders was detected via SCN loss, somatic mutations, and transcriptomics. Upregulation of genes in the AURKA pathway are consistent with the activation of MYC regulated genes in nonresponders. Several genes in the AKT1 axis had increased mutation rate in nonresponders. We also found evidence of resistance via PDCD1 overexpression in responders.
Finally, we identified candidates drugs to reverse AA/P resistance: topoisomerase inhibitors and drugs targeting the cell cycle via the MYC/AURKA/AURKB/TOP2A and/or PI3K_AKT_MTOR pathways.
我们在前列腺癌医学优化基因组增强治疗(PROMOTE)研究中鉴定了转移性去势抵抗性前列腺癌(mCRPC)患者对阿比特龙醋酸盐/泼尼松(AA/P)的耐药机制。我们分析了 83 例转移性活检患者在 AA/P 治疗 12 周前后(V1 和 V2)的全外显子测序(WES)和 RNA 测序数据。耐药性通过治疗改变时间(TTTC)确定。在 V2 时,58 例患者中有 18 例和 11 例患者分别表现出短期(中位 3.6 个月;范围 1.4-4.5)或长期(中位 29 个月;范围 23.5-41.7)反应。无反应者 TGFBR3 表达水平较低,Wnt 通路、细胞周期激活增加,AR 变体在上和治疗后上调,治疗后 AR 抑制剂 CDK11B 进一步缺失。无反应者在治疗后观察到雄激素处理基因 HSD17B11 和 CYP19A1 的缺失。在 V2 时,应答者和无应答者之间的细胞周期、DNA 修复、Wnt 信号和 Aurora 激酶途径相关基因的表达存在差异。通过 SCN 缺失、体细胞突变和转录组学检测到无反应者中 Wnt 信号的激活和有反应者中 MYC 或其靶基因的失活。AURKA 途径中基因的上调与无反应者中 MYC 调节基因的激活一致。无反应者中 AKT1 轴的几个基因突变率增加。我们还在应答者中发现了通过 PDCD1 过表达产生耐药性的证据。
最后,我们确定了逆转 AA/P 耐药性的候选药物:拓扑异构酶抑制剂和靶向细胞周期的药物,通过 MYC/AURKA/AURKB/TOP2A 和/或 PI3K_AKT_MTOR 通路。