Jiao Jia, Wang Li, Ni Fenfen, Wang Mo, Feng Shipin, Gao Xiaojie, Chan Han, Yang Xueying, Lee Hao, Chi Huan, Chen Xuelan, Wu Daoqi, Zhang Gaofu, Yang Baohui, Wang Anshuo, Yang Qin, Wan Junli, Yu Sijie, Li Xiaoqin, Wang Mei, Chen Xiaofeng, Mai Xianying, Ruan Xiongzhong, Yang Haiping, Li Qiu
Department of Nephrology, Children's Hospital of Chongqing Medical University, National Clinical Research Center for Child Health and Disorders, Ministry of Education Key Laboratory of Child Development and Disorders, Chongqing Key Laboratory of Pediatrics, Chongqing 400015, PR China.
Department of Nephrology, Chengdu Women and Children Central Hospital, Chengdu, Sichuan 610091, PR China.
Genes Dis. 2022 May 5;9(6):1662-1673. doi: 10.1016/j.gendis.2022.03.023. eCollection 2022 Nov.
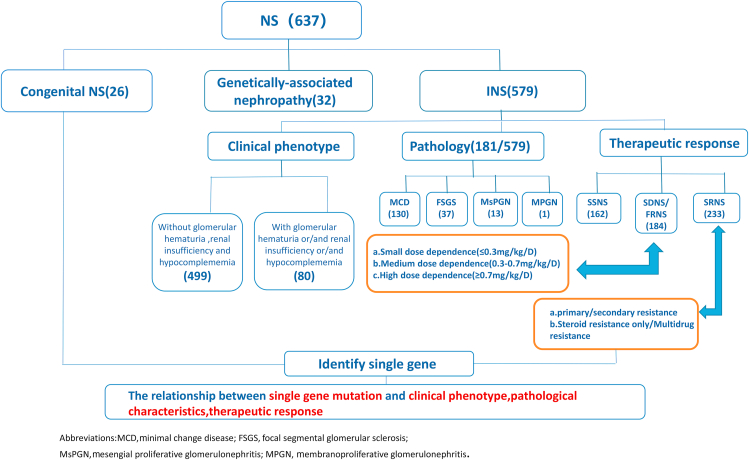
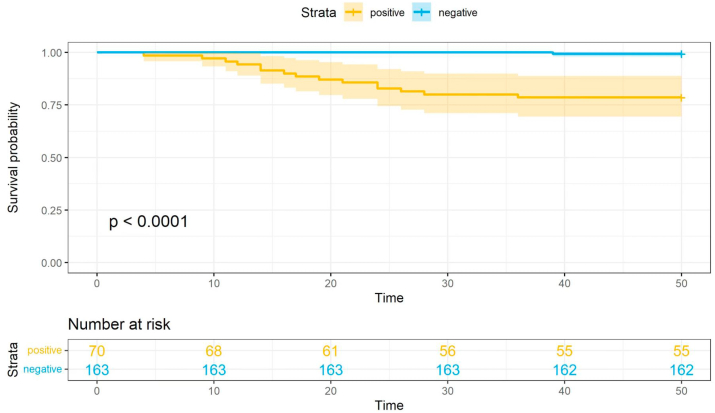
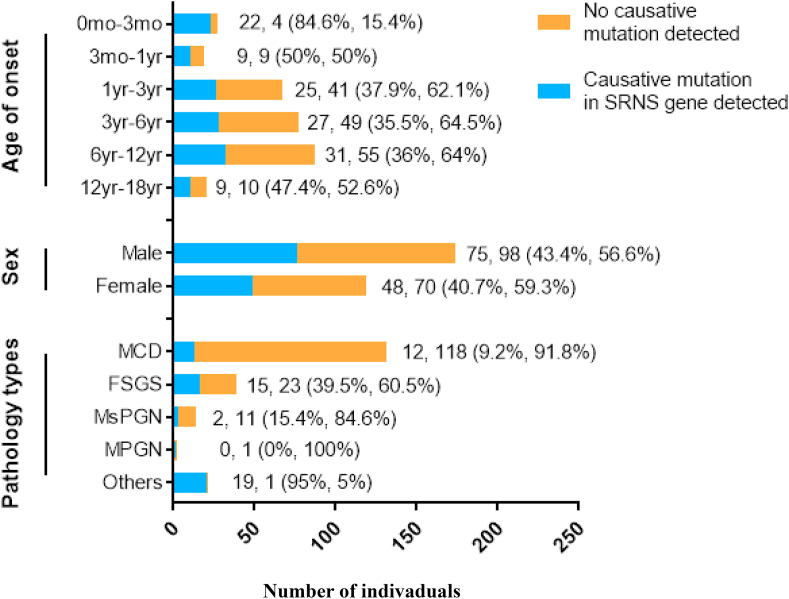
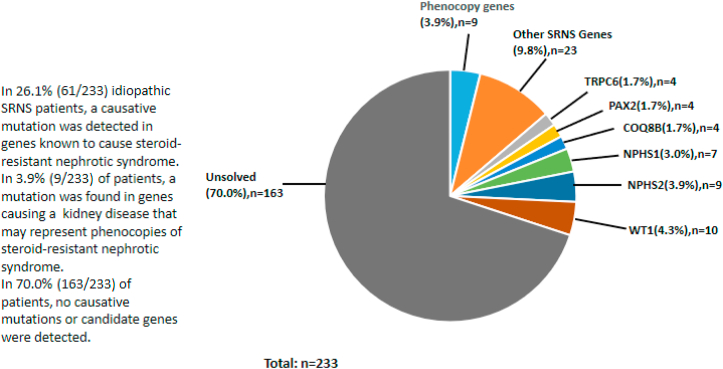
Understanding the association between the genetic and clinical phenotypes in children with nephrotic syndrome (NS) of different etiologies is critical for early clinical guidance. We employed whole-exome sequencing (WES) to detect monogenic causes of NS in a multicenter cohort of 637 patients. In this study, a genetic cause was identified in 30.0% of the idiopathic steroid-resistant nephrotic syndrome (SRNS) patients. Other than congenital nephrotic syndrome (CNS), there were no significant differences in the incidence of monogenic diseases based on the age at manifestation. Causative mutations were detected in 39.5% of patients with focal segmental glomerulosclerosis (FSGS) and 9.2% of those with minimal change disease (MCD). In terms of the patterns in patients with different types of steroid resistance, a single gene mutation was identified in 34.8% of patients with primary resistance, 2.9% with secondary resistance, and 71.4% of children with multidrug resistance. Among the various intensified immunosuppressive therapies, tacrolimus (TAC) showed the highest response rate, with 49.7% of idiopathic SRNS patients achieving complete remission. Idiopathic SRNS patients with monogenic disease showed a similar multidrug resistance pattern, and only 31.4% of patients with monogenic disease achieved a partial remission on TAC. During an average 4.1-year follow-up, 21.4% of idiopathic SRNS patients with monogenic disease progressed to end-stage renal disease (ESRD). Collectively, this study provides evidence that genetic testing is necessary for presumed steroid-resistant and idiopathic SRNS patients, especially those with primary and/or multidrug resistance.
了解不同病因的儿童肾病综合征(NS)的基因与临床表型之间的关联对于早期临床指导至关重要。我们采用全外显子组测序(WES)在一个637例患者的多中心队列中检测NS的单基因病因。在本研究中,30.0%的特发性类固醇抵抗性肾病综合征(SRNS)患者被确定有基因病因。除先天性肾病综合征(CNS)外,基于发病年龄的单基因疾病发病率无显著差异。在局灶节段性肾小球硬化(FSGS)患者中,39.5%检测到致病突变,微小病变病(MCD)患者中为9.2%。就不同类型类固醇抵抗患者的模式而言,在原发性抵抗患者中,34.8%鉴定出单基因突变,继发性抵抗患者中为2.9%,多药抵抗儿童中为71.4%。在各种强化免疫抑制治疗中,他克莫司(TAC)显示出最高的缓解率,49.7%的特发性SRNS患者实现完全缓解。患有单基因疾病的特发性SRNS患者表现出相似的多药抵抗模式,且仅有31.4%的单基因疾病患者使用TAC后实现部分缓解。在平均4.1年的随访中,21.4%患有单基因疾病的特发性SRNS患者进展为终末期肾病(ESRD)。总体而言,本研究提供了证据表明,对于疑似类固醇抵抗和特发性SRNS患者,尤其是那些具有原发性和/或多药抵抗的患者,基因检测是必要的。