Lang Jiachun, Wang Chen, Wang Le, Zhang Jingxia, Hu Yuecheng, Sun Huajun, Cong Hongliang, Liu Yin
Clinical School of Thoracic, Tianjin Medical University, Tianjin, China.
Department of Cardiology, Tianjin Chest Hospital, Tianjin, China.
Front Cardiovasc Med. 2022 Sep 9;9:943323. doi: 10.3389/fcvm.2022.943323. eCollection 2022.
Studies have highlighted the significant role of staged percutaneous coronary intervention (PCI) for a multivessel disease (MVD) among patients with ST-elevation myocardial infarction (STEMI). However, the relative benefit of staged vs. culprit-only PCI for MVD in elderly patients with STEMI remains undetermined. Thus, the present study compared the clinical outcomes of staged and culprit-only PCI in this cohort.
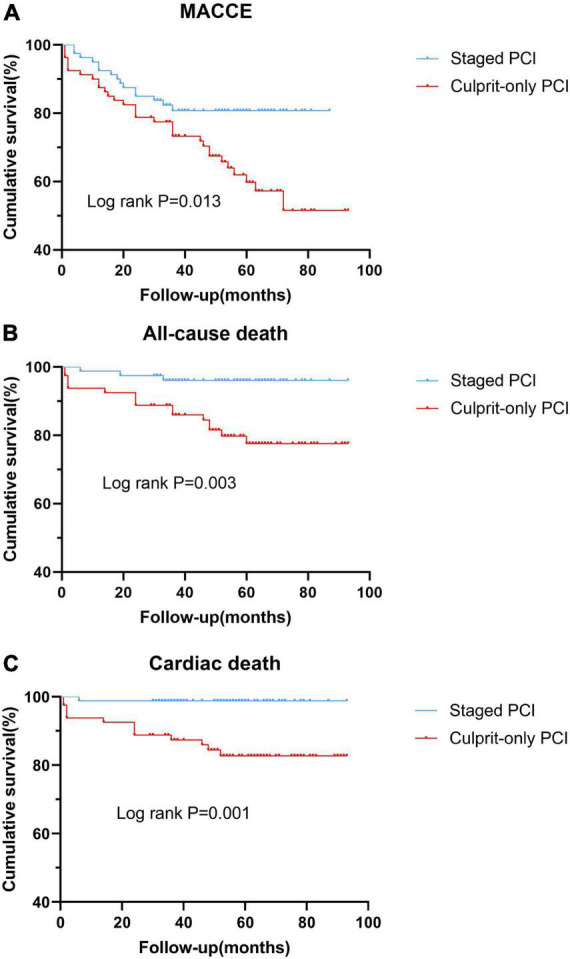
From January 2014 to September 2019, 617 patients aged ≥65 years with STEMI and MVD who underwent primary PCI of the culprit vessels within 12 h of symptom onset were enrolled. They were then categorized into the staged and culprit-only PCI groups according to intervention strategy. Propensity score matching (PSM) was conducted to adjust for confounding factors between groups. The primary end point was major adverse cardiac and cerebrovascular events (MACCE), a composite of all-cause death, cardiac death, recurrent myocardial infarction (MI), stroke, and ischemia-driven revascularization.
During a mean follow-up of 56 months, 209 patients experienced MACCE and 119 died. Staged revascularization was associated with a lower risk of MACCE, all-cause death, and cardiac death than culprit-only PCI in both overall patients and the PSM cohorts. In contrast, there was no significant difference in stroke or ischemia-driven revascularization. Moreover, on multivariate Cox regression analysis, staged PCI was a significant predictor of a lower incidence of MACCE and all-cause death.
In elderly patients with STEMI and MVD, staged PCI is superior to culprit-only PCI.
研究强调了分期经皮冠状动脉介入治疗(PCI)在ST段抬高型心肌梗死(STEMI)患者多支血管病变(MVD)中的重要作用。然而,在老年STEMI患者中,分期PCI与仅对罪犯血管进行PCI治疗MVD的相对获益仍未确定。因此,本研究比较了该队列中分期PCI与仅对罪犯血管进行PCI的临床结局。
纳入2014年1月至2019年9月期间617例年龄≥65岁、患有STEMI和MVD且在症状发作12小时内接受了罪犯血管直接PCI的患者。然后根据干预策略将他们分为分期PCI组和仅对罪犯血管进行PCI组。采用倾向评分匹配(PSM)来调整组间的混杂因素。主要终点是主要不良心脑血管事件(MACCE),包括全因死亡、心源性死亡、再发心肌梗死(MI)、中风和缺血驱动的血运重建。
在平均56个月的随访期间,209例患者发生MACCE,119例死亡。在总体患者和PSM队列中,分期血运重建与仅对罪犯血管进行PCI相比,MACCE、全因死亡和心源性死亡风险更低。相比之下,中风或缺血驱动的血运重建方面无显著差异。此外,多因素Cox回归分析显示,分期PCI是MACCE和全因死亡发生率较低的显著预测因素。
在老年STEMI和MVD患者中,分期PCI优于仅对罪犯血管进行PCI。