From the Department of Neurology (J.R.R., H.J.A.), Boston University School of Medicine, MA; Department of Biostatistics (A.P. S.D.), Boston University School of Public Health, MA; Department of Neurology (C.S.D.), University of California at Davis, CA; The Glenn Biggs Institute for Alzheimer's and Neurodegenerative Diseases (S.S.), University of Texas Health Sciences Center, San Antonio, TX; and NHLBI's Framingham Heart Study (J.R.R., A.P., H.J.A., S.D., S.S.), MA.
Neurology. 2022 Dec 5;99(23):e2561-e2571. doi: 10.1212/WNL.0000000000201293.
Perivascular spaces (PVS) visible on MRI scans may represent key aspects in the pathophysiology of stroke and dementia, including cerebral small vessel disease and glymphatic dysfunction. This study aimed to determine the association between MRI-visible PVS burden and the risk of incident dementia.
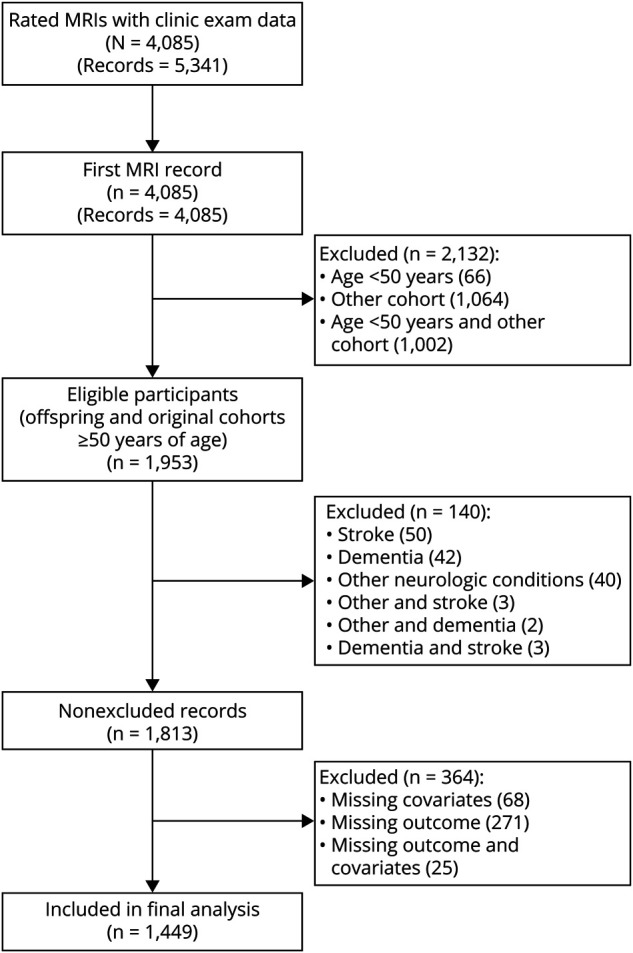
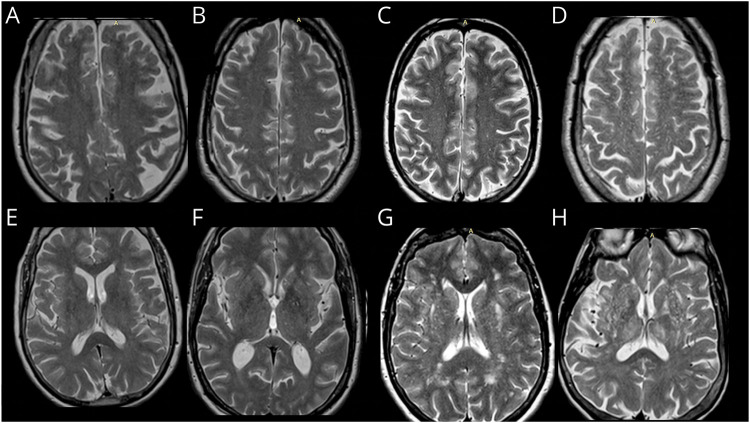
This study included community-dwelling Framingham Heart Study Original and Offspring cohort participants with available brain MRI-PVS ratings, free of stroke and dementia. Multivariable Cox proportional hazard regression was used to obtain hazard ratios (HRs) and 95% CIs of the association between MRI-visible PVS and incident dementia. PVS were rated using validated methods in the basal ganglia (BG) and centrum semiovale (CSO). The outcomes included all-cause dementia, Alzheimer dementia (AD), and vascular dementia (VaD).
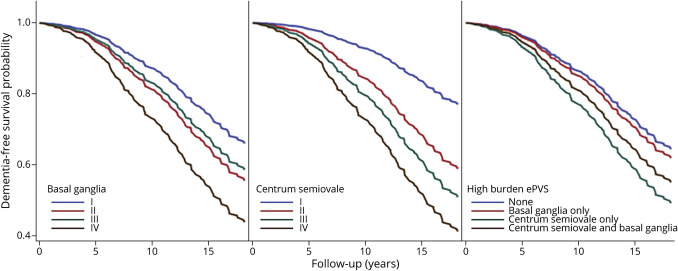
One thousand four hundred forty-nine participants 50 years or older (46% male) were included. Over a median follow-up period of 8.3 years, the incidence of all-cause dementia, AD, and VaD was 15.8%, 12.5%, and 2.5%, respectively. In models that adjusted for vascular risk factors and cardiovascular disease, the hazard for dementia increased steadily as PVS burden increased, rising 2-fold for those with grade II PVS (HR 2.44, 95% CI 1.51-3.93) to 5-fold in participants with grade IV (HR 5.05, 95% CI 2.75-9.26) compared with grade I PVS in CSO. In the BG, hazards increased 1.6-fold (HR 1.62, 95% CI 1.15-2.27) for grade II to 2.6-fold (HR 2.67, 95% CI 1.04-6.88) for grade IV compared with grade I PVS. The association remained significant for CSO but not for BG, after adjustment for white matter hyperintensity volume (WMHV), covert infarcts, and total brain volume. Similar findings were observed for AD, but VaD, limited by a small number of events, was not statistically significant.
Higher burden of PVS in CSO was associated with increased risk of developing dementia, independent of vascular risk factors, total brain volume, WMHVs, and covert infarcts. This finding supports a role for PVS as a subclinical MRI marker to identify individuals in subclinical stages at high risk of developing dementia who may benefit from early intervention.
磁共振成像(MRI)扫描中可见的血管周围间隙(PVS)可能代表中风和痴呆病理生理学中的关键方面,包括脑小血管疾病和糖质淋系统功能障碍。本研究旨在确定 MRI 可见 PVS 负担与痴呆症发病风险之间的关联。
本研究纳入了Framingham 心脏研究原队列和后代队列中居住在社区的参与者,这些参与者具有可用的脑 MRI-PVS 评分,且无中风和痴呆。采用多变量 Cox 比例风险回归分析评估 MRI 可见 PVS 与新发痴呆之间的关联。使用基底节(BG)和半卵圆中心(CSO)的验证方法对 PVS 进行评分。结局包括全因痴呆、阿尔茨海默病痴呆(AD)和血管性痴呆(VaD)。
本研究共纳入了 1449 名 50 岁及以上(46%为男性)的参与者。在中位随访 8.3 年期间,全因痴呆、AD 和 VaD 的发生率分别为 15.8%、12.5%和 2.5%。在调整血管危险因素和心血管疾病的模型中,随着 PVS 负担的增加,痴呆的风险呈稳步上升趋势,CSO 中 PVS 分级 II 级(HR 2.44,95%CI 1.51-3.93)和 IV 级(HR 5.05,95%CI 2.75-9.26)的风险分别是 PVS 分级 I 级的 2 倍和 5 倍。在 BG 中,PVS 分级 II 级(HR 1.62,95%CI 1.15-2.27)和 IV 级(HR 2.67,95%CI 1.04-6.88)的风险分别是 PVS 分级 I 级的 1.6 倍和 2.6 倍。在调整脑白质高信号容积(WMHV)、隐匿性梗死和总脑容量后,CSO 中这种关联仍然显著,但在 BG 中则不显著。类似的发现也见于 AD,但由于事件数量有限,VaD 无统计学意义。
CSO 中 PVS 负担的增加与痴呆风险的增加相关,这独立于血管危险因素、总脑容量、WMHV 和隐匿性梗死。这一发现支持 PVS 作为一种亚临床 MRI 标志物的作用,可用于识别处于亚临床阶段、痴呆风险较高的个体,这些个体可能受益于早期干预。