Buscho Seth E, Ishihara Rhys, Gupta Praveena K, Mopuru Renuka
Department of Ophthalmology and Visual Sciences, University of Texas Medical Branch, Galveston, USA.
Cureus. 2022 Aug 27;14(8):e28465. doi: 10.7759/cureus.28465. eCollection 2022 Aug.
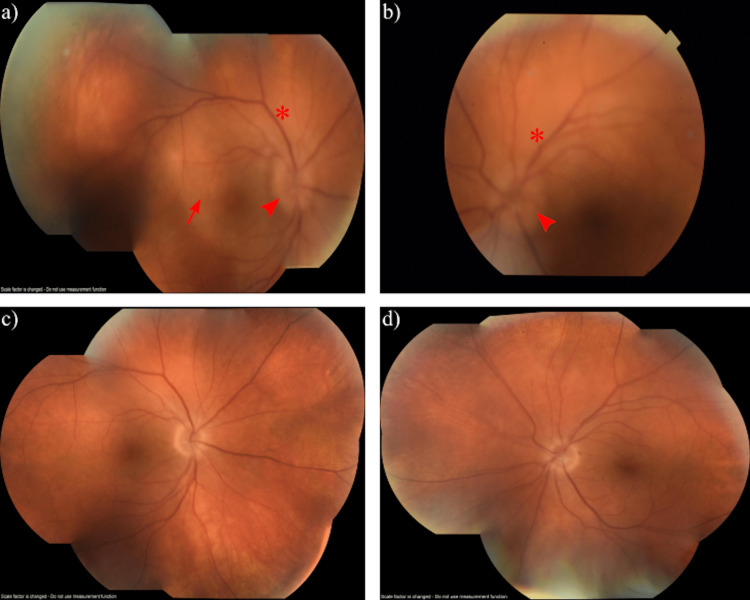
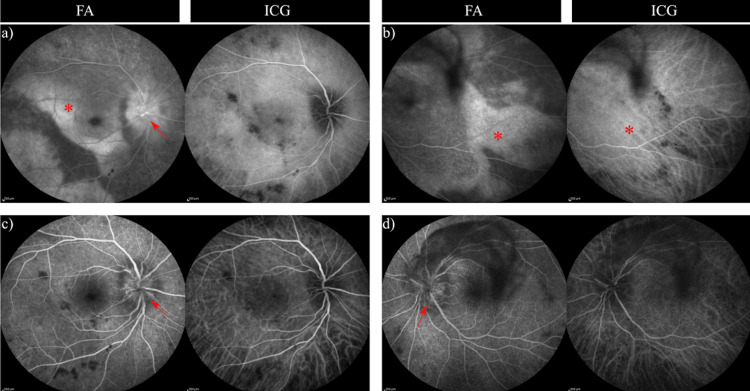
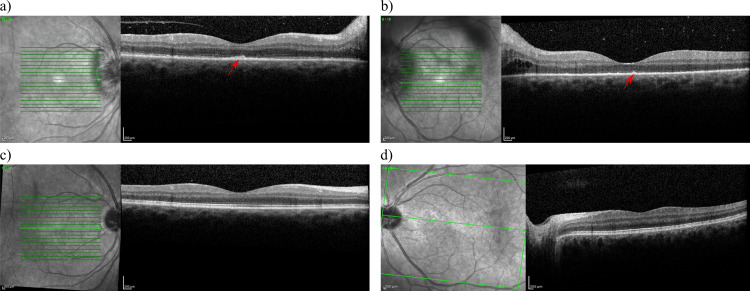
Ocular syphilis is a common presentation for patients with secondary or tertiary syphilis and usually includes posterior uveitis or panuveitis, though a myriad of symptoms have been associated. We report the case of a 58-year-old Caucasian male who presented with fast-progressing vision loss and a new onset of floaters in both eyes. An initial fundus exam revealed only bilateral optic disc edema, and neurological evaluation was negative. Subsequent ophthalmology evaluation in the clinic revealed a ragged retinal pigmented epithelium on optical coherence tomography (OCT) and posterior placoid chorioretinitis, raising suspicion of syphilis. Intravenous penicillin therapy was immediately initiated based on high clinical suspicion of ocular syphilis while awaiting lab confirmation, which was later confirmed as a new syphilis infection. He was subsequently given oral prednisone 48 hours into penicillin therapy for a significant posterior inflammatory response in both his eyes. His visual recovery was drastic due to the timely use of oral steroids. Classical findings such as ragged retinal pigmented epithelium on OCT and posterior placoid chorioretinitis demonstrate strong clinical suspicion of ocular syphilis. Oral prednisone when used timely with penicillin therapy in special situations such as bilateral severe posterior uveitis, panuveitis, or optic neuritis may aid in a faster and smoother visual recovery. A high index of clinical suspicion of ocular syphilis should be maintained in patients with human immunodeficiency virus (HIV) infection presenting with uveitis, posterior placoid morphology, or optic disc edema. Oral prednisone may be an effective adjuvant treatment for immunocompetent patients who mount a strong inflammatory response to ocular syphilis infection.
眼部梅毒是二期或三期梅毒患者的常见表现,通常包括后葡萄膜炎或全葡萄膜炎,不过也有多种相关症状。我们报告一例58岁的白种男性病例,该患者出现快速进展的视力丧失且双眼新发飞蚊症。初次眼底检查仅发现双侧视盘水肿,神经学评估为阴性。随后在诊所进行的眼科评估显示,光学相干断层扫描(OCT)检查发现视网膜色素上皮参差不齐,以及后极部扁平状脉络膜视网膜炎,这引发了对梅毒的怀疑。基于高度怀疑眼部梅毒,在等待实验室确诊期间立即开始静脉注射青霉素治疗,后来确诊为新的梅毒感染。在青霉素治疗48小时后,因其双眼出现明显的后部炎症反应,给他使用了口服泼尼松。由于及时使用了口服类固醇,他的视力恢复显著。OCT检查发现视网膜色素上皮参差不齐以及后极部扁平状脉络膜视网膜炎等典型表现,强烈提示眼部梅毒。在双侧严重后葡萄膜炎、全葡萄膜炎或视神经炎等特殊情况下,口服泼尼松与青霉素治疗同时及时使用,可能有助于视力更快、更顺利地恢复。对于出现葡萄膜炎、后极部形态异常或视盘水肿的人类免疫缺陷病毒(HIV)感染患者,应高度怀疑眼部梅毒。口服泼尼松对于对眼部梅毒感染产生强烈炎症反应的免疫功能正常患者可能是一种有效的辅助治疗方法。