Faculty of Medicine, University of Helsinki, Helsinki, Finland.
Finnish Medical Society Duodecim, Helsinki, Finland.
Implement Sci. 2022 Oct 1;17(1):65. doi: 10.1186/s13012-022-01238-z.
Healthcare costs are rising, and a substantial proportion of medical care is of little value. De-implementation of low-value practices is important for improving overall health outcomes and reducing costs. We aimed to identify and synthesize randomized controlled trials (RCTs) on de-implementation interventions and to provide guidance to improve future research.
MEDLINE and Scopus up to May 24, 2021, for individual and cluster RCTs comparing de-implementation interventions to usual care, another intervention, or placebo. We applied independent duplicate assessment of eligibility, study characteristics, outcomes, intervention categories, implementation theories, and risk of bias.
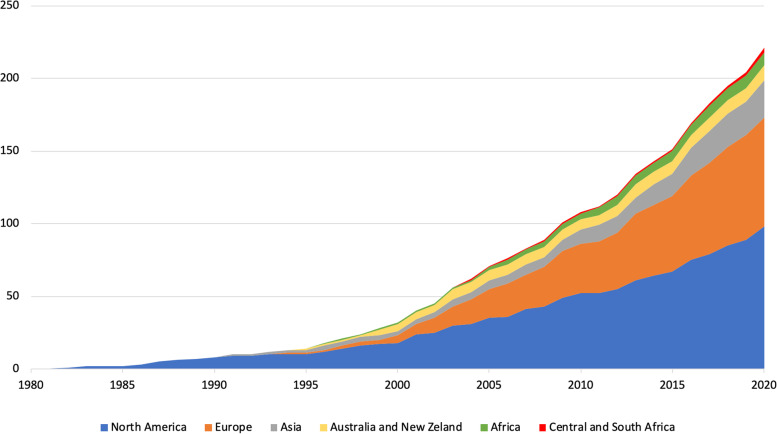
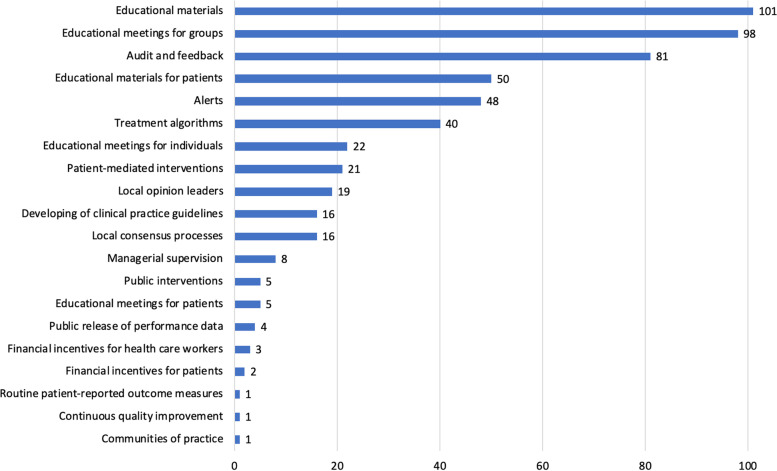
Of the 227 eligible trials, 145 (64%) were cluster randomized trials (median 24 clusters; median follow-up time 305 days), and 82 (36%) were individually randomized trials (median follow-up time 274 days). Of the trials, 118 (52%) were published after 2010, 149 (66%) were conducted in a primary care setting, 163 (72%) aimed to reduce the use of drug treatment, 194 (85%) measured the total volume of care, and 64 (28%) low-value care use as outcomes. Of the trials, 48 (21%) described a theoretical basis for the intervention, and 40 (18%) had the study tailored by context-specific factors. Of the de-implementation interventions, 193 (85%) were targeted at physicians, 115 (51%) tested educational sessions, and 152 (67%) multicomponent interventions. Missing data led to high risk of bias in 137 (60%) trials, followed by baseline imbalances in 99 (44%), and deficiencies in allocation concealment in 56 (25%).
De-implementation trials were mainly conducted in primary care and typically aimed to reduce low-value drug treatments. Limitations of current de-implementation research may have led to unreliable effect estimates and decreased clinical applicability of studied de-implementation strategies. We identified potential research gaps, including de-implementation in secondary and tertiary care settings, and interventions targeted at other than physicians. Future trials could be improved by favoring simpler intervention designs, better control of potential confounders, larger number of clusters in cluster trials, considering context-specific factors when planning the intervention (tailoring), and using a theoretical basis in intervention design.
OSF Open Science Framework hk4b2.
医疗保健成本不断上升,相当一部分医疗服务的价值较低。淘汰低价值实践对于改善整体健康结果和降低成本非常重要。我们旨在确定和综合淘汰干预措施的随机对照试验(RCT),并为改进未来的研究提供指导。
截至 2021 年 5 月 24 日,我们对 MEDLINE 和 Scopus 进行了检索,以查找比较淘汰干预措施与常规护理、其他干预措施或安慰剂的个体和群组 RCT。我们独立重复评估了合格性、研究特征、结果、干预类别、实施理论和偏倚风险。
在 227 项合格试验中,145 项(64%)为群组随机试验(中位数 24 个群组;中位数随访时间 305 天),82 项(36%)为个体随机试验(中位数随访时间 274 天)。这些试验中,118 项(52%)发表于 2010 年以后,149 项(66%)在初级保健环境中进行,163 项(72%)旨在减少药物治疗的使用,194 项(85%)测量了护理总用量,64 项(28%)将低价值护理使用作为结果。这些试验中,48 项(21%)描述了干预措施的理论基础,40 项(18%)根据特定环境因素对研究进行了调整。淘汰干预措施中,193 项(85%)针对医生,115 项(51%)测试了教育课程,152 项(67%)为多组分干预措施。由于数据缺失,137 项(60%)试验的偏倚风险较高,其次是 99 项(44%)的基线失衡,56 项(25%)的分配隐藏缺陷。
淘汰试验主要在初级保健中进行,通常旨在减少低价值药物治疗。当前淘汰研究的局限性可能导致不可靠的效果估计和研究中淘汰策略的临床适用性降低。我们确定了潜在的研究差距,包括在二级和三级保健环境中的淘汰以及针对非医生的干预措施。未来的试验可以通过采用更简单的干预设计、更好地控制潜在混杂因素、在群组试验中增加更多的群组、在干预计划(调整)中考虑特定环境因素以及在干预设计中使用理论基础来改进。
OSF 开放科学框架 hk4b2。