Hilal Lara, Wu Abraham J, Reyngold Marsha, Cuaron John J, Navilio John, Romesser Paul B, Dreyfuss Alexandra, Yin Sean, Zhang Zhigang, Bai Xing, Berry Sean L, Zinovoy Melissa, Nusrat Maliha, Pappou Emmanouil, Zelefsky Michael J, Crane Christopher H, Hajj Carla
Department of Radiation Oncology, American University of Beirut Medical Center, Beirut, Lebanon.
Department of Radiation Oncology, Memorial Sloan Kettering Cancer Center, New York, NY, United States.
Front Oncol. 2022 Sep 15;12:975519. doi: 10.3389/fonc.2022.975519. eCollection 2022.
Radiation therapy (RT) for anorectal cancer after prior prostate cancer RT is usually avoided due to concern for complications. Data on this topic is scarce. Our aim was to evaluate tolerability, toxicity, and clinical outcomes associated with a second course of pelvic radiation in men with anorectal cancers previously treated with RT for prostate cancer.
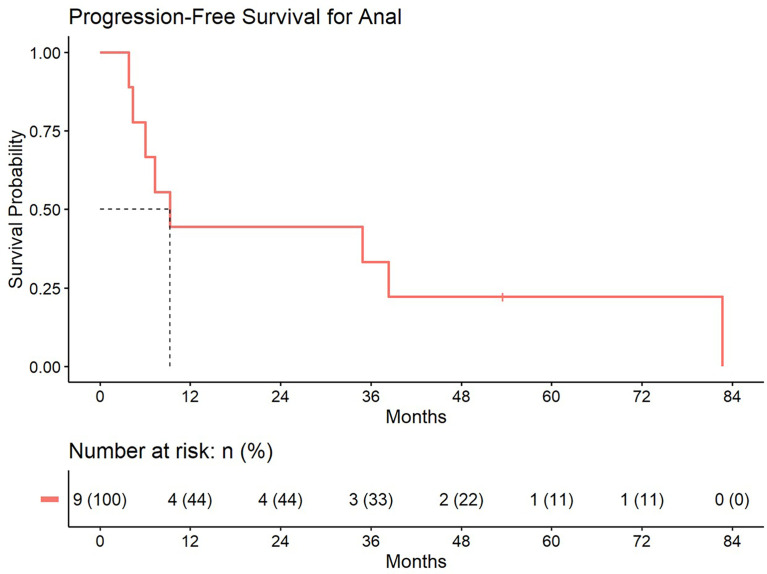
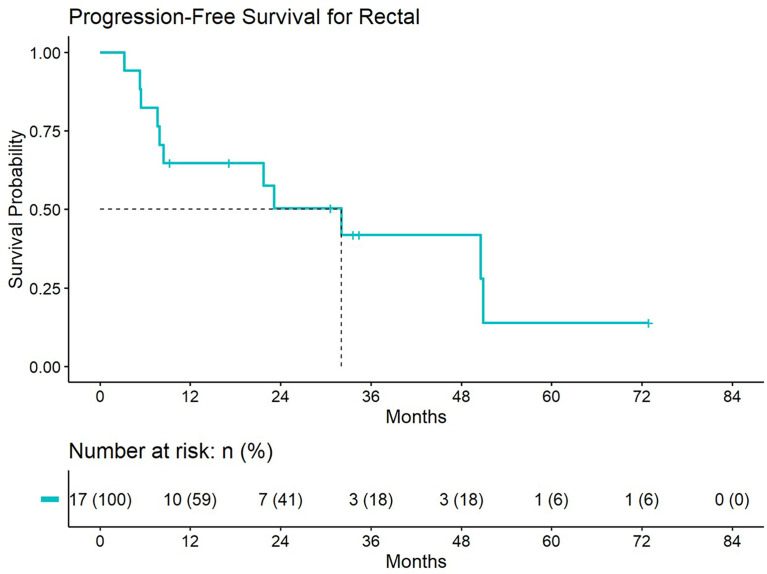
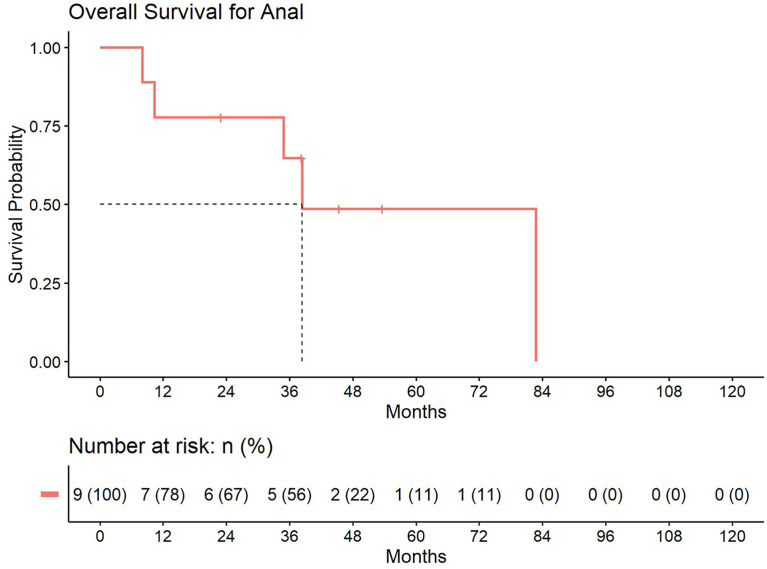
MATERIALS/METHODS: We conducted a single-institution retrospective study of men treated with RT for rectal or anal cancer after prior prostate RT. Toxicity data were collected. Treatment plans were extracted to assess doses to organs at risk and target coverage. Cumulative incidence was calculated for local and distant progression. Kaplan-Meier curves were used to estimate overall survival (OS) and progression-free survival (PFS).
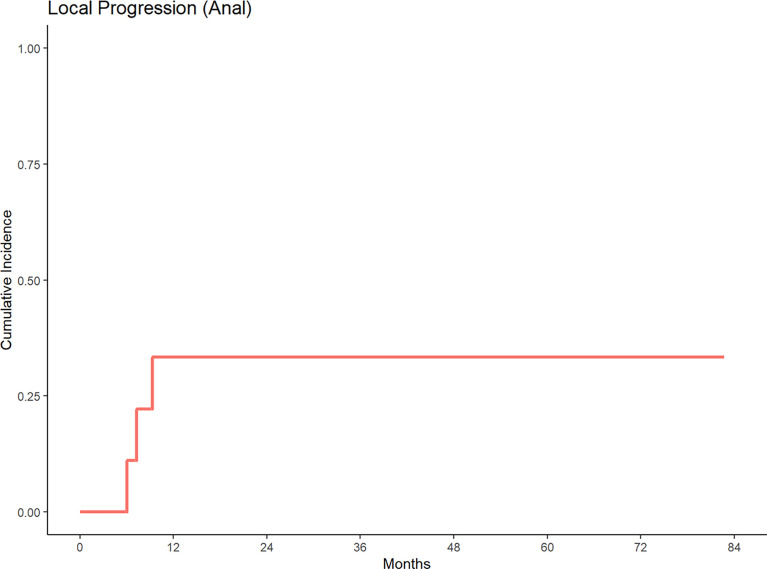
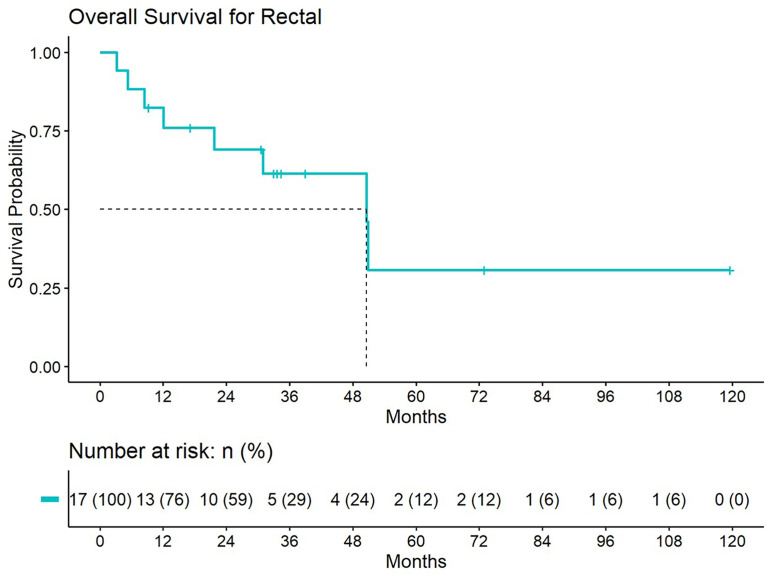
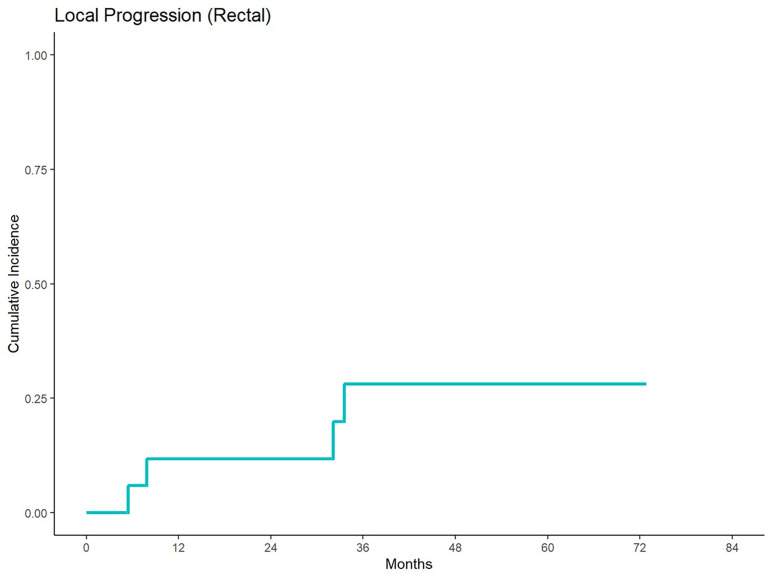
We identified 26 patients who received anorectal RT after prostate cancer RT: 17 for rectal cancer and 9 for anal cancer. None had metastatic disease. Prior prostate RT was delivered using low dose rate brachytherapy (LDR), external beam RT (EBRT), or EBRT + LDR. RT for rectal cancer was delivered most commonly using 50.4Gy/28 fractions (fr) or 1.5 Gy twice-daily to 30-45 Gy. The most used RT dose for anal cancer was 50Gy/25 fr. Median interval between prostate and anorectal RT was 12.3 years (range:0.5 - 25.3). 65% and 89% of rectal and anal cancer patients received concurrent chemotherapy, respectively. There were no reported ≥Grade 4 acute toxicities. Two patients developed fistulae; one was urinary-cutaneous after prostate LDR and 45Gy/25fr for rectal cancer, and the other was recto-vesicular after prostate LDR and 50Gy/25fr for anal cancer. In 11 patients with available dosimetry, coverage for anorectal cancers was adequate. With a median follow up of 84.4 months, 5-yr local progression and OS were 30% and 31% for rectal cancer, and 35% and 49% for anal cancer patients, respectively.
RT for anorectal cancer after prior prostate cancer RT is feasible but should be delivered with caution since it poses a risk of fistulae and possibly bleeding, especially in patients treated with prior LDR brachytherapy. Further studies, perhaps using proton therapy and/or rectal hydrogel spacers, are needed to further decrease toxicity and improve outcomes.
由于担心并发症,通常避免对先前接受过前列腺癌放疗的患者进行肛管直肠癌的放射治疗(RT)。关于这个主题的数据很少。我们的目的是评估先前接受过前列腺癌放疗的男性患者进行第二轮盆腔放疗的耐受性、毒性和临床结果。
材料/方法:我们对先前接受过前列腺癌放疗后又接受直肠癌或肛管癌放疗的男性患者进行了单机构回顾性研究。收集了毒性数据。提取治疗计划以评估危及器官的剂量和靶区覆盖情况。计算局部和远处进展的累积发生率。使用Kaplan-Meier曲线估计总生存期(OS)和无进展生存期(PFS)。
我们确定了26例在前列腺癌放疗后接受肛管直肠癌放疗的患者:17例为直肠癌,9例为肛管癌。均无转移性疾病。先前的前列腺癌放疗采用低剂量率近距离放疗(LDR)、外照射放疗(EBRT)或EBRT+LDR。直肠癌放疗最常用的方案是50.4Gy/28分次(fr)或每日两次1.5Gy,总量达30-45Gy。肛管癌最常用的放疗剂量是50Gy/25fr。前列腺癌放疗与肛管直肠癌放疗的中位间隔时间为12.3年(范围:0.5-25.3年)。直肠癌和肛管癌患者分别有65%和89%接受了同步化疗。未报告≥4级急性毒性反应。两名患者出现瘘管;一例是在前列腺癌LDR和直肠癌45Gy/25fr放疗后出现尿皮肤瘘,另一例是在前列腺癌LDR和肛管癌50Gy/25fr放疗后出现直肠膀胱瘘。在11例有剂量测定数据的患者中,肛管直肠癌的靶区覆盖情况良好。中位随访84.4个月,直肠癌患者5年局部进展率和总生存率分别为30%和31%,肛管癌患者分别为35%和49%。
先前接受过前列腺癌放疗的患者进行肛管直肠癌放疗是可行的,但应谨慎进行,因为存在瘘管形成和可能出血的风险,尤其是在先前接受过LDR近距离放疗的患者中。可能需要进一步的研究,或许采用质子治疗和/或直肠水凝胶间隔物,以进一步降低毒性并改善治疗效果。