Institute for Global Health, University College London, London, UK.
Royal Free London NHS Foundation Trust, London, UK.
J Viral Hepat. 2023 Jan;30(1):46-55. doi: 10.1111/jvh.13757. Epub 2022 Nov 2.
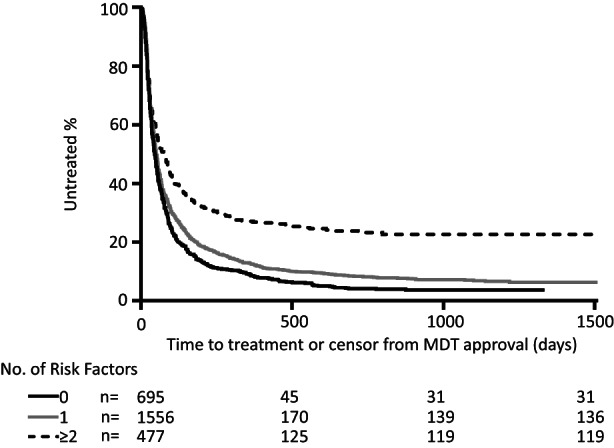
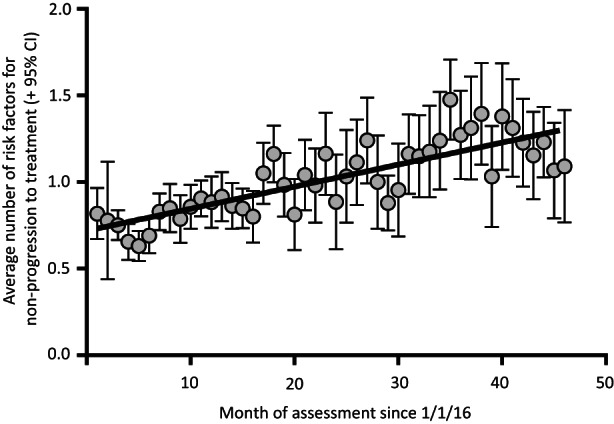
Most high-income countries are not on track to achieve the World Health Organization hepatitis C elimination targets. As elimination programmes assess growing proportions of patients in community-based pathways, rates of treatment uptake may fall. We aimed to identify factors associated with DAA treatment uptake and measure changes in their prevalence over time. We performed a time-to-treatment analysis on 2728 patients approved for hepatitis C Direct-Acting Antiviral treatment in the North Central London region between January 2016 and October 2019. We investigated the association between treatment uptake and factors including assessment/treatment setting (hospital, drug service or prison), patient age, gender, injection drug use, harmful alcohol use, cirrhosis status and previous treatment. The likelihood of treatment uptake was reduced by three independent risk factors. These included assessment setting: prison-based or drug-service pathways (aHR 0.29 or 0.81 vs. hospital outpatient pathway, 95% CI 0.21-0.40 and 0.70-0.94 respectively, p < .001); being UK-born (aHR 0.89 vs. non-UK born, 0.82-0.98, p = .01); and history of harmful alcohol use (aHR 0.84 vs. no history, 0.72-0.99, p = .04). The average number of these risk factors for not starting treatment per patient increased over time (R = 0.66 p < .001). Independent of these, there was an additional 5% reduction in rate of treatment initiation in each successive year of the programme (aHR 0.95, 0.91-0.99, p = .02). In conclusion, disengagement from care before treatment uptake was found to be a growing threat to elimination. Despite provision of community-based test-to-cure pathways, there are persistent barriers to treatment uptake and these are increasing over time.
大多数高收入国家都无法实现世界卫生组织的丙型肝炎消除目标。随着消除规划评估越来越多的患者采用社区途径,治疗的接受率可能会下降。我们旨在确定与 DAA 治疗接受率相关的因素,并衡量其随时间的变化。我们对 2016 年 1 月至 2019 年 10 月期间在伦敦北部中部地区获得丙型肝炎直接作用抗病毒治疗批准的 2728 名患者进行了治疗时间分析。我们调查了治疗接受率与评估/治疗设置(医院、药物服务或监狱)、患者年龄、性别、注射吸毒、有害饮酒、肝硬化状况和先前治疗等因素之间的关联。治疗接受率降低了三个独立的危险因素。其中包括评估设置:监狱或药物服务途径(aHR 0.29 或 0.81 与医院门诊途径相比,95%CI 0.21-0.40 和 0.70-0.94,p<0.001);英国出生(aHR 0.89 与非英国出生,0.82-0.98,p=0.01);以及有害饮酒史(aHR 0.84 与无历史,0.72-0.99,p=0.04)。每位患者未开始治疗的这些危险因素的平均数量随时间增加(R=0.66,p<0.001)。独立于这些因素,该计划的每一年都会使治疗开始率降低 5%(aHR 0.95,0.91-0.99,p=0.02)。总之,在开始治疗之前脱离治疗被发现是消除的一个日益严重的威胁。尽管提供了基于社区的检测到治愈途径,但仍然存在治疗接受率的持续障碍,并且这些障碍随时间的推移而增加。