Hubert Elizabeth, Dains Joyce E
The University of Texas MD Anderson Cancer Center, Houston, Texas.
J Adv Pract Oncol. 2022 Sep;13(7):695-704. doi: 10.6004/jadpro.2022.13.7.5. Epub 2022 Oct 12.
The purpose of this integrative review was to establish the role of cardiac rhythm analysis (electrocardiogram; EKG) and echocardiogram in increasing clinical suspicion for and earlier diagnosis of cardiac amyloidosis.
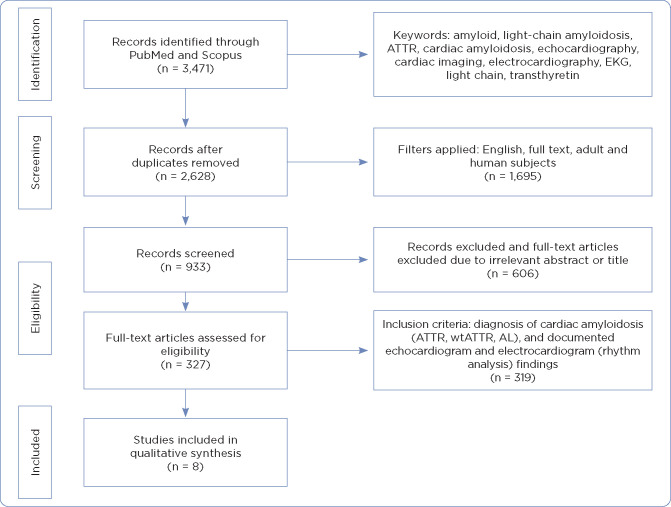
A literature review was conducted using PubMed and Scopus databases. Dates searched were from January 2017 to May 2021. Inclusion criteria included a diagnosis of cardiac amyloidosis, use of EKG, and echocardiogram participants 18 years and older. Articles were excluded if they were duplicates, had an irrelevant title, or were incomplete.
Results indicated neither EKG nor echocardiogram alone or in combination are sufficient for diagnosing cardiac amyloidosis. There is, however, a combination of findings that could potentially prove useful in "ruling in" cardiac amyloidosis and prompt further evaluation. Predominant findings in cardiac amyloidosis cohorts found on EKG showed low-voltage QRS complexes, a pseudo-infarct pattern in precordial leads, and an absence of left ventricular hypertrophy on EKG. There is no single echocardiogram finding specific to cardiac amyloidosis. Patients will generally present with thickened ventricular walls, and nearly all patients will display a preserved left ventricular ejection fraction until later stages of disease. Strain imaging, either via 2D or 3D transthoracic echocardiogram, is more useful in screening for or detecting cardiac amyloidosis and should be utilized in this instance. Findings in cardiac amyloidosis include decreased global longitudinal strain and relative apical sparing.
Overall, EKG and echocardiogram are effective, feasible, and practical tools to increase clinical suspicion for cardiac amyloidosis for the purposes of early recognition and evaluation. These are useful only to "rule in" a diagnosis. Future studies are needed to validate these findings.
本整合性综述的目的是确定心律分析(心电图;EKG)和超声心动图在提高对心脏淀粉样变性的临床怀疑及早期诊断方面的作用。
使用PubMed和Scopus数据库进行文献综述。检索日期为2017年1月至2021年5月。纳入标准包括心脏淀粉样变性的诊断、EKG的使用以及年龄在18岁及以上的超声心动图参与者。如果文章是重复的、标题不相关或不完整,则将其排除。
结果表明,单独使用EKG或超声心动图,或两者联合使用,都不足以诊断心脏淀粉样变性。然而,有一组发现可能有助于“确诊”心脏淀粉样变性并促使进一步评估。在EKG上发现的心脏淀粉样变性队列中的主要表现为QRS波群低电压、胸前导联的假性梗死模式以及EKG上无左心室肥厚。没有单一的超声心动图表现是心脏淀粉样变性所特有的。患者通常会出现心室壁增厚,几乎所有患者在疾病后期之前左心室射血分数都会保持正常。通过二维或三维经胸超声心动图进行的应变成像在筛查或检测心脏淀粉样变性方面更有用,在此情况下应予以使用。心脏淀粉样变性的表现包括整体纵向应变降低和相对心尖保留。
总体而言,EKG和超声心动图是有效的、可行的和实用的工具,可提高对心脏淀粉样变性的临床怀疑,以进行早期识别和评估。这些仅有助于“确诊”诊断。需要未来的研究来验证这些发现。