Center for Immuno-Oncology, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD.
Collaborative Bioinformatics Resource, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD.
Blood. 2023 Feb 9;141(6):659-672. doi: 10.1182/blood.2022016660.
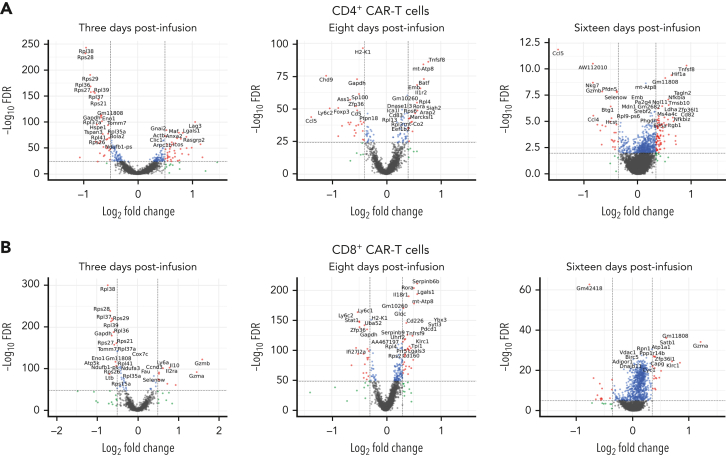
Relapse limits the therapeutic efficacy both of chimeric antigen receptor (CAR) T cells and allogeneic hematopoietic cell transplantation (allo-HCT). Patients may undergo these therapies sequentially to prevent or treat relapsed malignancy. However, direct integration of the 2 therapies has been avoided over concerns for potential induction of graft-versus-host disease (GVHD) by allogeneic CAR T cells. We have shown in murine T-cell-replete MHC-haploidentical allo-HCT that suppressive mechanisms induced immediately after posttransplant cyclophosphamide (PTCy), given on days +3/+4, prevent GVHD induction by alloreactive T cells infused as early as day +5. Therefore, we hypothesized that allogeneic CAR T cells given in a similarly integrated manner in our murine MHC-haploidentical allo-HCT model may safely exert antitumor effects. Indeed, allogeneic anti-CD19 CAR T cells given early after (day +5) PTCy or even prior to (day 0) PTCy cleared leukemia without exacerbating the cytokine release syndrome occurring from the MHC-haploidentical allo-HCT or interfering with PTCy-mediated GVHD prevention. Meanwhile, CAR T-cell treatment on day +9 or day +14 was safe but less effective, suggesting a limited therapeutic window. CAR T cells infused before PTCy were not eliminated, but surviving CAR T cells continued to proliferate highly and expand despite PTCy. In comparison with infusion on day +5, CAR T-cell infusion on day 0 demonstrated superior clinical efficacy associated with earlier CAR T-cell expansion, higher phenotypic CAR T-cell activation, less CD4+CD25+Foxp3+ CAR T-cell recovery, and transcriptional changes suggesting increased activation of CD4+ CAR T cells and more cytotoxic CD8+ CAR T cells. This study provides mechanistic insight into PTCy's impact on graft-versus-tumor immunity and describes novel approaches to integrate CAR T cells and allo-HCT that may compensate for deficiencies of each individual approach.
复发限制了嵌合抗原受体 (CAR) T 细胞和同种异体造血细胞移植 (allo-HCT) 的治疗效果。为了预防或治疗复发的恶性肿瘤,患者可能会先后接受这些治疗。然而,由于担心同种异体 CAR T 细胞可能会引发移植物抗宿主病 (GVHD),一直避免直接整合这两种治疗方法。我们在小鼠 T 细胞丰富的 MHC 单倍体不全 allo-HCT 中表明,在移植后环磷酰胺 (PTCy) 给予的第 3/4 天给予抑制性机制,可预防早在第 5 天输注同种反应性 T 细胞引发的 GVHD。因此,我们假设在我们的 MHC 单倍体不全 allo-HCT 模型中以类似的方式给予同种异体 CAR T 细胞可能会安全地发挥抗肿瘤作用。事实上,在 PTCy 后早期(第+5 天)或甚至在 PTCy 之前(第 0 天)给予同种异体抗 CD19 CAR T 细胞可清除白血病,而不会加重由 MHC 单倍体不全 allo-HCT 引起的细胞因子释放综合征或干扰 PTCy 介导的 GVHD 预防。同时,第+9 天或第+14 天给予 CAR T 细胞治疗是安全的,但效果较差,提示治疗窗口有限。在 PTCy 之前给予的 CAR T 细胞未被消除,但存活的 CAR T 细胞继续高度增殖和扩增,尽管存在 PTCy。与第+5 天输注相比,第 0 天输注 CAR T 细胞表现出更好的临床疗效,与 CAR T 细胞更早的扩增、更高的表型 CAR T 细胞激活、更少的 CD4+CD25+Foxp3+CAR T 细胞恢复以及提示 CD4+CAR T 细胞激活增加和更多细胞毒性 CD8+CAR T 细胞的转录变化相关。这项研究提供了关于 PTCy 对移植物抗肿瘤免疫影响的机制见解,并描述了整合 CAR T 细胞和 allo-HCT 的新方法,这些方法可能弥补每种方法的不足。