Experimental Transplantation and Immunology Branch, Center for Cancer Research, National Cancer Institute, National Institutes of Health, Bethesda, MD, United States.
Front Immunol. 2019 Nov 29;10:2668. doi: 10.3389/fimmu.2019.02668. eCollection 2019.
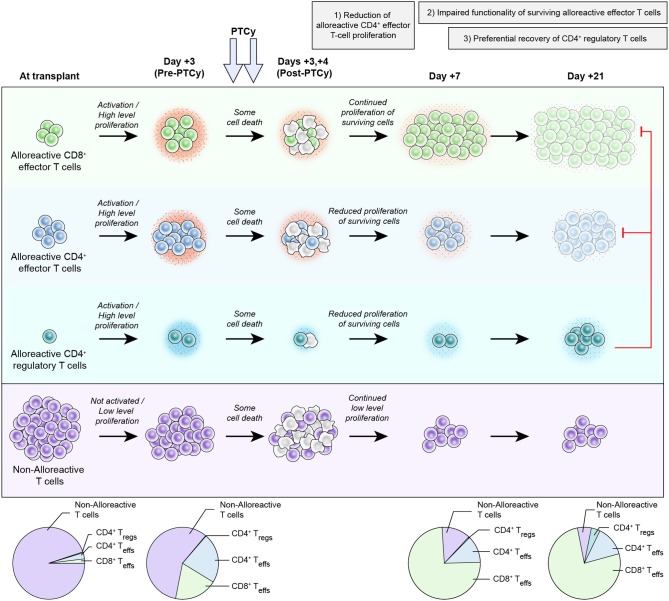
Post-transplantation cyclophosphamide (PTCy) has been highly successful at preventing severe acute and chronic graft-versus-host disease (GVHD) after allogeneic hematopoietic cell transplantation (HCT). The clinical application of this approach was based on extensive studies in major histocompatibility complex (MHC)-matched murine skin allografting models, in which cyclophosphamide was believed to act via three main mechanisms: (1) selective elimination of alloreactive T cells; (2) intrathymic clonal deletion of alloreactive T-cell precursors; and (3) induction of suppressor T cells. In these models, cyclophosphamide was only effective in very specific contexts, requiring particular cell dose, cell source, PTCy dose, and recipient age. Achievement of transient mixed chimerism also was required. Furthermore, these studies showed differences in the impact of cyclophosphamide on transplanted cells (tumor) versus tissue (skin grafts), including the ability of cyclophosphamide to prevent rejection of the former but not the latter after MHC-mismatched transplants. Yet, clinically PTCy has demonstrated efficacy in MHC-matched or partially-MHC-mismatched HCT across a wide array of patients and HCT platforms. Importantly, clinically significant acute GVHD occurs frequently after PTCy, inconsistent with alloreactive T-cell elimination, whereas PTCy is most active against severe acute GVHD and chronic GVHD. These differences between murine skin allografting and clinical HCT suggest that the above-mentioned mechanisms may not be responsible for GVHD prevention by PTCy. Indeed, recent work by our group in murine HCT has shown that PTCy does not eliminate alloreactive T cells nor is the thymus necessary for PTCy's efficacy. Instead, other mechanisms appear to be playing important roles, including: (1) reduction of alloreactive CD4 effector T-cell proliferation; (2) induced functional impairment of surviving alloreactive CD4 and CD8 effector T cells; and (3) preferential recovery of CD4 regulatory T cells. Herein, we review the history of cyclophosphamide's use in preventing murine skin allograft rejection and our evolving new understanding of the mechanisms underlying its efficacy in preventing GVHD after HCT. Efforts are ongoing to more fully refine and elaborate this proposed new working model. The completion of this effort will provide critical insight relevant for the rational design of novel approaches to improve outcomes for PTCy-treated patients and for the induction of tolerance in other clinical contexts.
移植后环磷酰胺(PTCy)在预防异基因造血细胞移植(HCT)后严重的急性和慢性移植物抗宿主病(GVHD)方面非常成功。这种方法的临床应用是基于在主要组织相容性复合体(MHC)匹配的鼠皮肤同种异体移植模型中的广泛研究,其中环磷酰胺被认为通过三种主要机制起作用:(1)选择性消除同种反应性 T 细胞;(2)同种反应性 T 细胞前体的胸腺内克隆删除;和(3)诱导抑制性 T 细胞。在这些模型中,环磷酰胺仅在特定情况下有效,需要特定的细胞剂量、细胞来源、PTCy 剂量和受者年龄。还需要实现短暂的混合嵌合体。此外,这些研究表明环磷酰胺对移植细胞(肿瘤)与组织(皮肤移植物)的影响存在差异,包括环磷酰胺预防前者排斥但不预防后者排斥 MHC 错配移植后的能力。然而,临床上 PTCy 在广泛的患者和 HCT 平台上已证明在 MHC 匹配或部分 MHC 不匹配的 HCT 中有效。重要的是,PTCy 后经常发生临床上明显的急性 GVHD,与同种反应性 T 细胞消除不一致,而 PTCy 对严重急性 GVHD 和慢性 GVHD 最有效。这些在鼠皮肤同种异体移植和临床 HCT 之间的差异表明,上述机制可能不是 PTCy 预防 GVHD 的原因。事实上,我们小组在鼠 HCT 中的最新工作表明,PTCy 不会消除同种反应性 T 细胞,胸腺对于 PTCy 的疗效也不是必需的。相反,其他机制似乎发挥着重要作用,包括:(1)减少同种反应性 CD4 效应 T 细胞的增殖;(2)诱导存活的同种反应性 CD4 和 CD8 效应 T 细胞的功能障碍;和(3)优先恢复 CD4 调节性 T 细胞。在此,我们回顾了环磷酰胺在预防鼠皮肤同种异体移植排斥中的应用历史,并介绍了我们对其在预防 HCT 后 GVHD 中的疗效机制的不断深入理解。目前正在努力更全面地完善和阐述这个提出的新工作模式。这项工作的完成将为合理设计新方法提供关键的见解,以改善 PTCy 治疗患者的预后,并在其他临床情况下诱导耐受。