Pharmacoepidemiology and Risk Management, RTI Health Solutions, Barcelona, Spain.
Pharmacoepidemiology and Risk Management, RTI Health Solutions, Waltham, MA, USA.
BMC Geriatr. 2022 Oct 6;22(1):784. doi: 10.1186/s12877-022-03489-3.
Little is known about the incidence of clinical events and treatment patterns among older adults with dementia-related psychosis. Given that dementia-related psychosis comprises various dementia types, this study describes the incidence of clinical events and treatment patterns by dementia type after patients with dementia are diagnosed with psychosis.
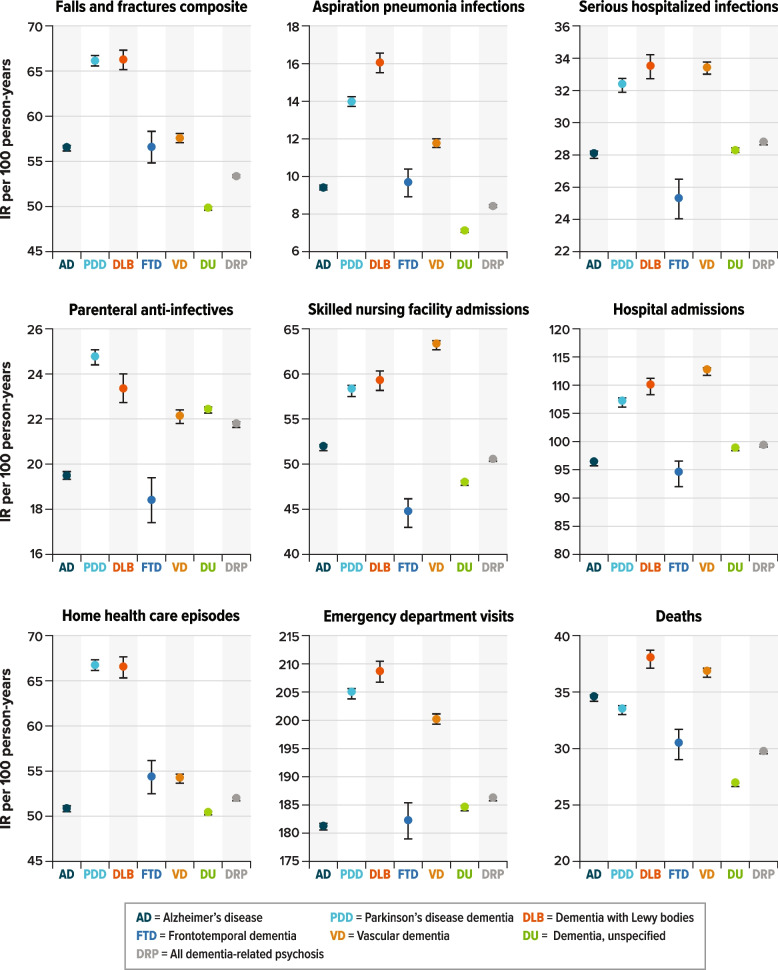
Adults aged ≥ 65 years with dementia and newly diagnosed with psychosis were identified in US Medicare claims during 2013-2018. Baseline characteristics were evaluated at the time of the psychosis diagnosis. After the initial psychosis diagnosis, incidence rates (IRs) of clinical events (e.g., falls/fractures, infections, healthcare utilization), mortality, and patterns of antipsychotic treatment were described for each dementia type (Alzheimer's disease [AD], Parkinson's disease dementia [PDD], dementia with Lewy bodies [DLB], frontotemporal dementia [FTD], vascular dementia [VD], and unspecified dementia). Daily mean cumulative counts were estimated to describe the incidence of recurrent events over time. Mortality was described using Kaplan-Meier survival curves.
We identified 484,520 patients with dementia-related psychosis: mean age, 84 years (standard deviation, 7.8); female, 66%. At the time of psychosis diagnosis, the most prevalent type of dementia was unspecified dementia (56%), followed by AD (31%), VD (12%), PDD (10%), DLB (3%), and FTD (< 1%), and most patients had scores indicating severe illness on the Charlson Comorbidity Index (71%) and frailty index (62%). Across all dementia types, IRs (per 100 person-years) were high for emergency department visits, oral anti-infective use, and urinary tract infections after the initial psychosis diagnosis. Patients with DLB had the highest incidence of most clinical outcomes. After 1 year of follow-up, the cumulative probability of death was about 30% for all dementia types, and after 5 years, was about 80% among patients with DLB, VD, AD, or PDD and about 60%-65% among patients with FTD or unspecified dementia.
Patients with dementia-related psychosis had a high burden of comorbidities, frailty, emergency department visits, infections, and death. Specifically, after DRP diagnosis, patients with DLB and VD had the highest burden of clinical events of interest.
对于痴呆相关精神病患者的临床事件发生率和治疗模式知之甚少。鉴于痴呆相关精神病包括各种痴呆类型,本研究描述了在诊断为精神病后,根据痴呆类型发生的临床事件和治疗模式。
从美国医疗保险索赔中确定了 2013 年至 2018 年间年龄≥65 岁且新诊断为痴呆相关精神病的成年人。在精神病诊断时评估基线特征。在首次精神病诊断后,描述了每种痴呆类型(阿尔茨海默病 [AD]、帕金森病痴呆 [PDD]、路易体痴呆 [DLB]、额颞叶痴呆 [FTD]、血管性痴呆 [VD] 和未指定痴呆)的临床事件(如跌倒/骨折、感染、医疗保健利用)、死亡率和抗精神病药物治疗模式的发生率。通过每日平均累积计数来描述随时间复发事件的发生率。死亡率用 Kaplan-Meier 生存曲线来描述。
我们确定了 484520 例痴呆相关精神病患者:平均年龄 84 岁(标准差 7.8),女性占 66%。在精神病诊断时,最常见的痴呆类型是未指定的痴呆(56%),其次是 AD(31%)、VD(12%)、PDD(10%)、DLB(3%)和 FTD(<1%),大多数患者的 Charlson 合并症指数(71%)和脆弱指数(62%)得分表明病情严重。在所有痴呆类型中,在首次精神病诊断后,急诊就诊、口服抗感染药物使用和尿路感染的发生率(每 100 人年)较高。DLB 患者发生大多数临床结局的发生率最高。在 1 年的随访后,所有痴呆类型的死亡累积概率约为 30%,在 5 年后,DLB、VD、AD 或 PDD 患者的累积概率约为 80%,FTD 或未指定痴呆患者的累积概率约为 60%-65%。
痴呆相关精神病患者有较高的合并症、脆弱、急诊就诊、感染和死亡负担。具体来说,在诊断为 DRP 后,DLB 和 VD 患者发生感兴趣的临床事件的负担最高。