Otorhinolaryngology, Head and Neck Surgery, University Hospitals Leuven, Leuven, Belgium.
Department of Oncology, Section Head and Neck Oncology, KU Leuven, Leuven, Belgium.
Front Endocrinol (Lausanne). 2022 Sep 20;13:971249. doi: 10.3389/fendo.2022.971249. eCollection 2022.
Both anaplastic thyroid carcinoma (ATC) and thyroid lymphoma (TL) clinically present as rapidly enlarging neck masses. Unfortunately, in this situation, like in any other thyroid swelling, a routine fine-needle aspiration (FNA) cytology is the first and only diagnostic test performed at the initial contact in the average thyroid practice. FNA, however, has a low sensitivity in diagnosing ATC and TL, and by the time the often "inconclusive" result is known, precious time has evolved, before going for core-needle biopsy (CNB) or incisional biopsy (IB) as the natural next diagnostic steps.
To determine the diagnostic value of CNB in the clinical setting of a rapidly enlarging thyroid mass, a systematic review and meta-analysis of the available data on CNB reliability in the differential diagnosis of ATC and TL.
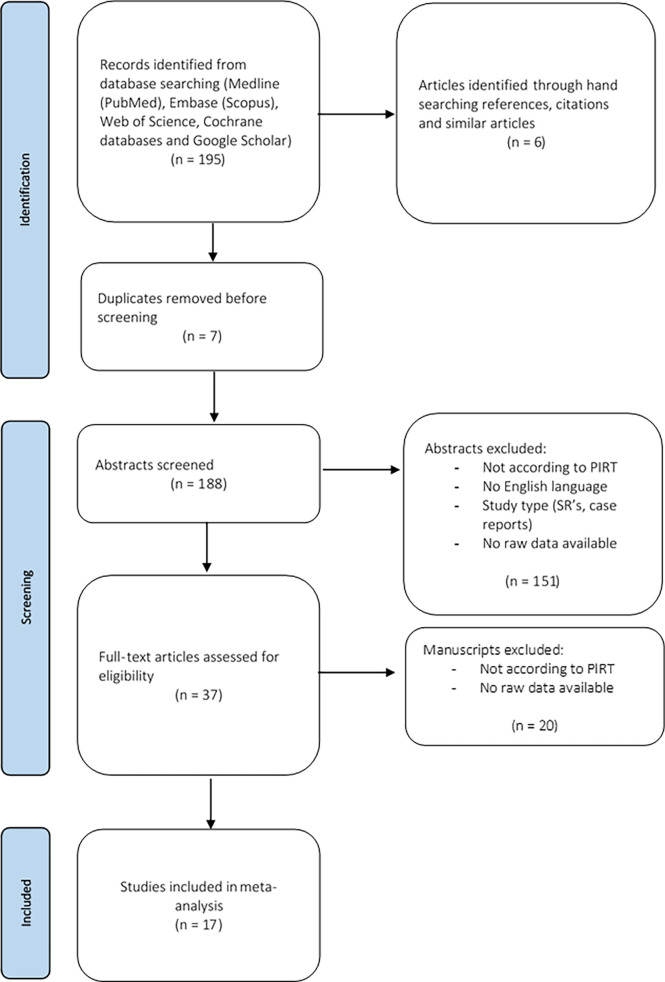
A PubMed, Embase and Web of Science database search was performed on June 23th 2021. Population of interest comprised patients who underwent CNB for clinical or ultrasonographical suspicion of ATC or TL, patients with a final diagnosis of ATC or TL after CNB, or after IB following CNB.
From a total of 17 studies, 166 patients were included. One hundred and thirty-six were diagnosed as TL and 14 as ATC following CNB. CNB, with a sensitivity and positive predictive value of 94,3% and 100% for TL and 80,1% and 100% for ATC respectively, proved to be superior to FNA (reported sensitivity for TL of 48% and for ATC of 61%). Furthermore, the need for additional diagnostic surgery after CNB was only 6.2% for TL and 17.6% for ATC.
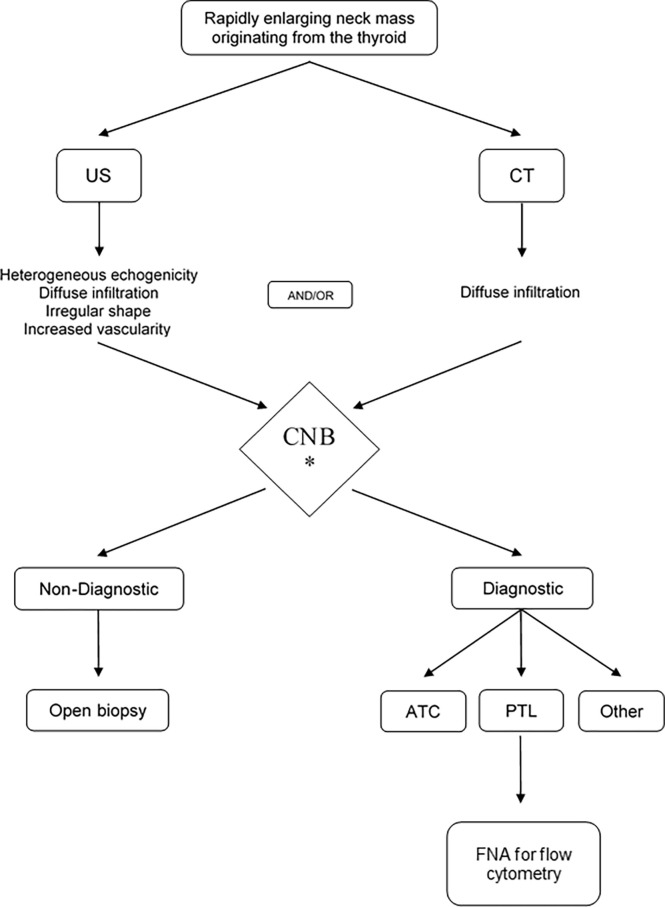
Immediately performing CNB for a suspected diagnosis of ATC and TL in a rapidly enlarging thyroid mass is more appropriate and straightforward than a stepped diagnostic pathway using FNA first and awaiting the result before doing CNB.
间变性甲状腺癌(ATC)和甲状腺淋巴瘤(TL)在临床上均表现为迅速增大的颈部肿块。不幸的是,在这种情况下,与任何其他甲状腺肿胀一样,在常规甲状腺实践中,初次接触时首先进行的也是唯一的诊断测试是常规细针抽吸(FNA)细胞学检查。然而,FNA 诊断 ATC 和 TL 的敏感性较低,并且在经常出现“不确定”结果时,已经浪费了宝贵的时间,然后才进行核心针活检(CNB)或切开活检(IB)作为自然的下一步诊断步骤。
确定 CNB 在快速增大的甲状腺肿块临床情况下的诊断价值,对 CNB 在 ATC 和 TL 鉴别诊断中的可靠性的现有数据进行系统评价和荟萃分析。
于 2021 年 6 月 23 日在 PubMed、Embase 和 Web of Science 数据库中进行了检索。研究对象包括因临床或超声检查怀疑 ATC 或 TL 而行 CNB 的患者、CNB 后最终诊断为 ATC 或 TL 的患者,或 CNB 后行 IB 的患者。
共纳入 17 项研究,总计 166 例患者。136 例患者诊断为 TL,14 例患者诊断为 ATC。CNB 对 TL 的敏感性和阳性预测值分别为 94.3%和 100%,对 ATC 的敏感性和阳性预测值分别为 80.1%和 100%,优于 FNA(报道的 TL 的敏感性为 48%,ATC 的敏感性为 61%)。此外,TL 患者行 CNB 后仅 6.2%需要进一步行诊断性手术,而 ATC 患者为 17.6%。
对于快速增大的甲状腺肿块疑似 ATC 和 TL 的诊断,立即进行 CNB 比首先进行 FNA 并在进行 CNB 之前等待结果的分步诊断方法更合适和直接。