Department of Internal Medicine, National Cancer Center, Goyang, Republic of Korea.
Department of Internal Medicine, Seoul National University Bundang Hospital and College of Medicine, Seongnam, Republic of Korea.
Thyroid. 2022 Nov;32(11):1328-1336. doi: 10.1089/thy.2021.0614.
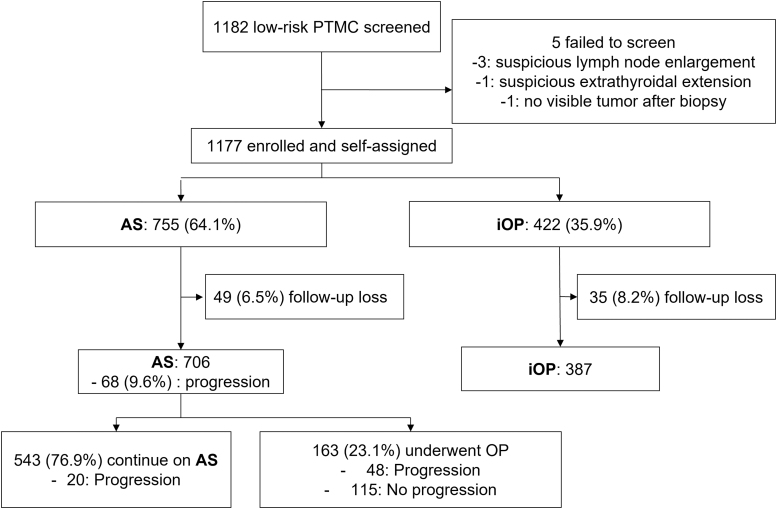
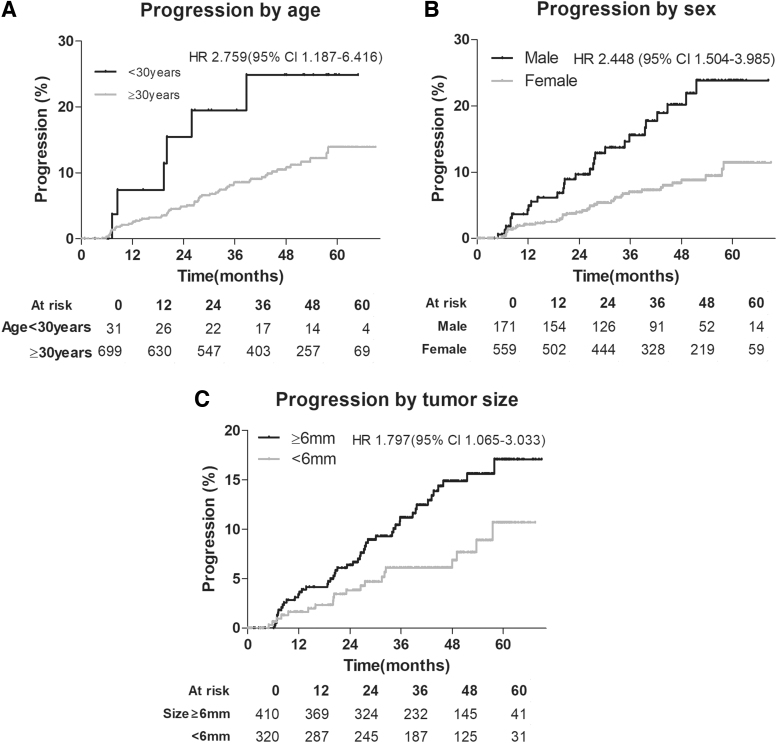
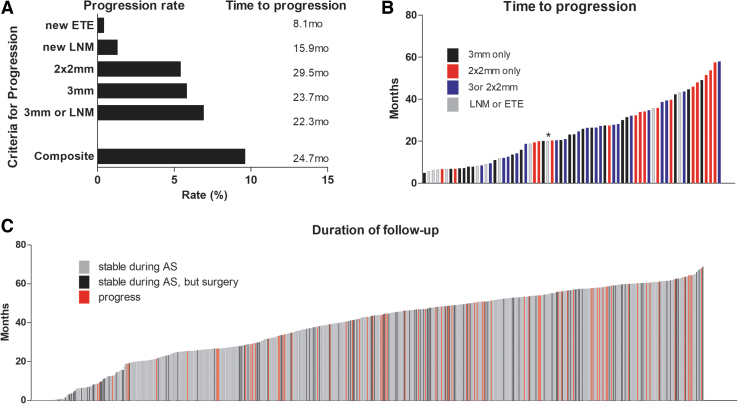
Active surveillance (AS) is an alternative to thyroidectomy for the management of low-risk papillary thyroid microcarcinoma (PTMC). However, prospective AS data collected from diverse populations are needed. This multicenter prospective cohort study enrolled patients from three referral hospitals in Korea. The participants were self-assigned into two groups, AS or immediate surgery. All patients underwent neck ultrasound every 6-12 months to monitor for disease progression. Progression under AS was evaluated by a criterion of tumor size increment by 3 mm in one dimension (3 mm), 2 mm in two dimensions (2 × 2 mm), new extrathyroidal extension (ETE), or new lymph node metastasis (LNM), and a composite outcome was defined using all four criteria. A total of 1177 eligible patients with PTMC (919 female, 78.1%) with a median age of 48 years (range 19-87) were enrolled; 755 (64.1%) patients chose AS and 422 (35.9%) underwent surgery. Among 755 patients under AS, 706 (female 537, 76.1%) underwent at least two ultrasound examinations and were analyzed. Over a follow-up period of 41.4 months (standard deviation, 16.0), 163 AS patients (23.1%) underwent surgery. Progression defined by the composite outcome was observed in 9.6% (68/706) of patients, and the 2- and 5-year progression estimates were 5.3% and 14.2%, respectively. The observed progression rates were 5.8% (41/706) and 5.4% (38/706) as defined by tumor size enlargement by 3 mm and 2 × 2 mm, respectively, and 1.3% (9/706) and 0.4% (3/706) for new LNM and ETE, respectively. No distant metastases developed during AS. In multivariate logistic regression analysis examining variables associated with progression under AS, age at diagnosis <30 years (odds ratio [OR], 2.86; 95% confidence interval [CI], 1.10 - 7.45), male sex (OR, 2.48; 95% CI, 1.47 - 4.20), and tumor size ≥6 mm (OR, 1.89; 95% CI, 1.09 - 3.27) were independently significant. The progression of low-risk PTMC during AS in the Korean population was low, but slightly higher than previously reported in other populations. Risk factors for disease progression under AS include younger age, male sex, and larger tumor size. Clinicaltrials.gov NCT02938702.
主动监测 (AS) 是治疗低危甲状腺微小乳头状癌 (PTMC) 的甲状腺切除术的替代方法。然而,需要从不同人群中收集前瞻性 AS 数据。本多中心前瞻性队列研究纳入了韩国三家转诊医院的患者。参与者自行分为 AS 或立即手术两组。所有患者每 6-12 个月进行一次颈部超声检查,以监测疾病进展情况。AS 下的进展通过肿瘤在一个维度上增加 3mm(3mm)、两个维度上增加 2mm(2×2mm)、新的甲状腺外延伸 (ETE) 或新的淋巴结转移 (LNM) 的标准来评估,并且使用所有四个标准定义复合结果。共有 1177 名符合条件的 PTMC 患者(919 名女性,78.1%),中位年龄为 48 岁(19-87 岁);755 名(64.1%)患者选择 AS,422 名(35.9%)接受手术。在 755 名接受 AS 的患者中,706 名(女性 537 名,76.1%)至少接受了两次超声检查并进行了分析。在 41.4 个月(标准差 16.0)的随访期间,163 名 AS 患者(23.1%)接受了手术。9.6%(68/706)的患者出现了复合结果定义的进展,2 年和 5 年的进展估计分别为 5.3%和 14.2%。肿瘤大小增大 3mm 和 2×2mm 分别观察到 5.8%(41/706)和 5.4%(38/706)的观察进展率,新的 LNM 和 ETE 分别为 1.3%(9/706)和 0.4%(3/706)。AS 期间未发生远处转移。在多变量逻辑回归分析中,检查与 AS 下进展相关的变量,诊断时年龄<30 岁(优势比 [OR],2.86;95%置信区间 [CI],1.10-7.45)、男性(OR,2.48;95% CI,1.47-4.20)和肿瘤大小≥6mm(OR,1.89;95% CI,1.09-3.27)是独立显著的。韩国人群中低危 PTMC 在 AS 期间的进展较低,但略高于其他人群的先前报告。AS 下疾病进展的危险因素包括年龄较小、男性和较大的肿瘤大小。Clinicaltrials.gov NCT02938702。