Laboratory of Molecular Biology, National Cancer Institute, National Institutes of Health, Bethesda, Maryland, USA.
Medical Oncology Program, National Cancer Institute, National Institutes of Health, Bethesda, Maryland, USA.
Cancer Med. 2023 Feb;12(4):4236-4249. doi: 10.1002/cam4.5290. Epub 2022 Oct 8.
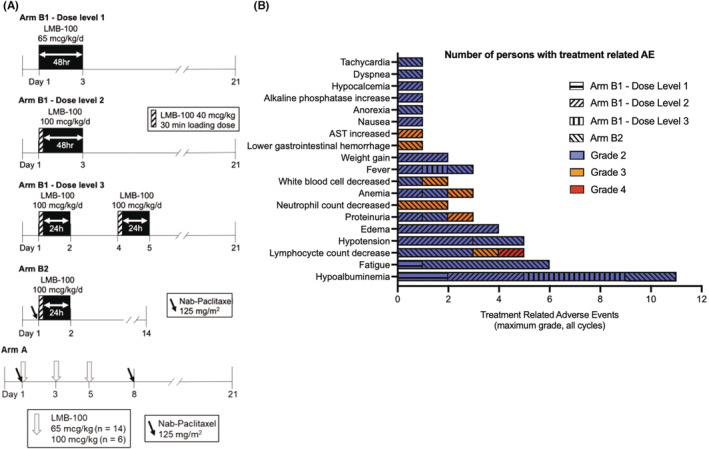
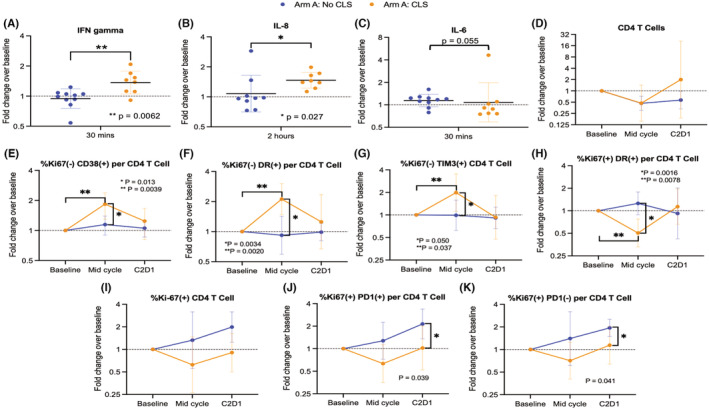
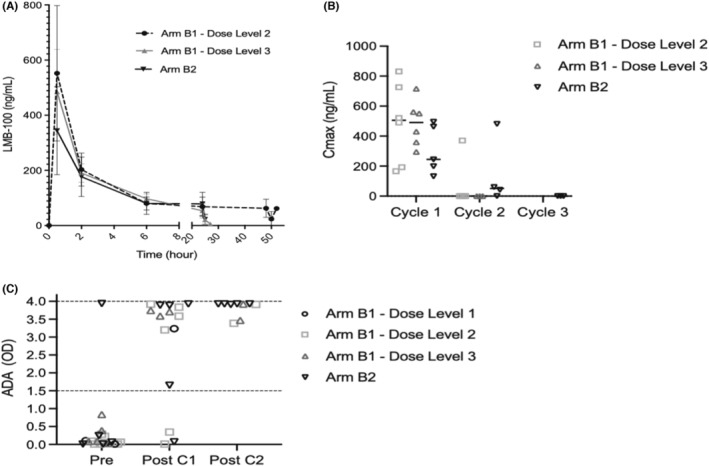
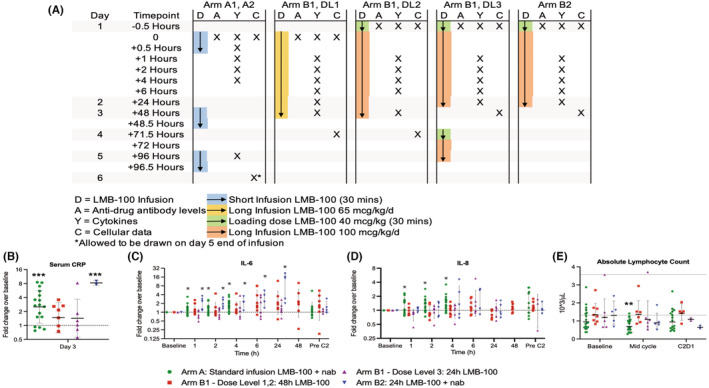
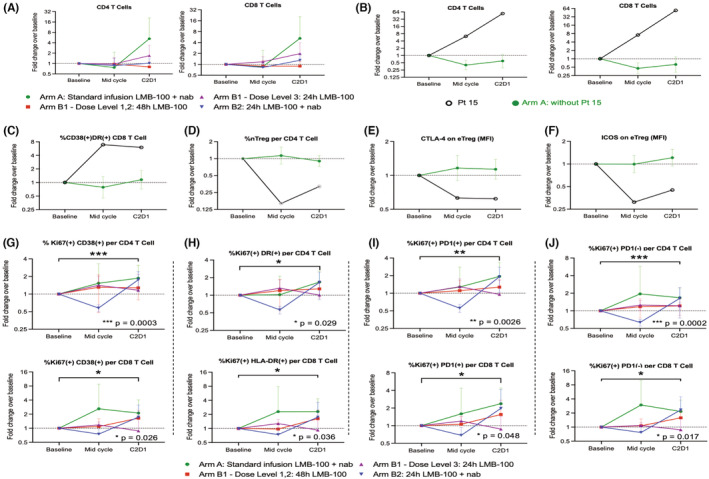
LMB-100 is a novel immune-conjugate (immunotoxin) that targets mesothelin. A phase 1/2 clinical trial was conducted (NCT02810418) with primary objectives assessing the safety and efficacy of LMB-100 ± nab-paclitaxel. Participant blood samples were analyzed for changes in serum cytokines and circulating immune cell subsets associated with response or toxicity. On Arm A, participants (n = 20) received standard 30-minute LMB-100 infusion with nab-paclitaxel. Although clinical efficacy was observed, the combination caused intolerable capillary leak syndrome (CLS), a major toxicity of unclear etiology that affects many immunotoxin drugs. Participants developing CLS experienced rapid elevations in IFNγ and IL-8 compared to those without significant CLS, along with midcycle increases in Ki-67- CD4 T cells that were CD38, HLA-DR, or TIM3 positive. Additionally, a strong increase in activated CD4 and CD8 T cells and a concurrent decrease in Tregs were seen in the single Arm A patient achieving a partial response. In Arm B, administration of single agent LMB-100 to participants (n = 20) as a long infusion given over 24-48 h was investigated based on pre-clinical data that this format could reduce CLS. An optimal dose and schedule of long infusion LMB-100 were identified, but no clinical efficacy was observed even in patients receiving LMB-100 in combination with nab-paclitaxel. Despite this, both Arm A and B participants experienced increases in specific subsets of proliferating CD4 and CD8 T cells following Cycle 1 treatment. In summary, LMB-100 treatment causes systemic immune activation. Inflammatory and immune changes that accompany drug associated CLS were characterized for the first time.
LMB-100 是一种针对间皮素的新型免疫偶联物(免疫毒素)。进行了一项 1/2 期临床试验(NCT02810418),主要目的是评估 LMB-100±nab-紫杉醇的安全性和疗效。对参与者的血液样本进行分析,以评估与反应或毒性相关的血清细胞因子和循环免疫细胞亚群的变化。在 Arm A 中,参与者(n=20)接受了标准的 30 分钟 LMB-100 输注,同时给予 nab-紫杉醇。虽然观察到了临床疗效,但该联合用药导致了无法耐受的毛细血管渗漏综合征(CLS),这是一种病因不明的主要毒性,影响许多免疫毒素药物。与没有明显 CLS 的参与者相比,发生 CLS 的参与者的 IFNγ和 IL-8 迅速升高,同时 Ki-67-CD4 T 细胞在中期增加,这些细胞呈 CD38、HLA-DR 或 TIM3 阳性。此外,在 Arm A 中,一名部分缓解的患者中观察到激活的 CD4 和 CD8 T 细胞显著增加,同时 Treg 减少。在 Arm B 中,基于临床前数据,研究了将单药 LMB-100 作为 24-48 小时的长输注给药用于参与者(n=20)的情况,该格式可以减少 CLS。确定了长输注 LMB-100 的最佳剂量和方案,但即使在接受 LMB-100 联合 nab-紫杉醇治疗的患者中也未观察到临床疗效。尽管如此,Arm A 和 B 的参与者在第 1 周期治疗后均经历了增殖性 CD4 和 CD8 T 细胞特定亚群的增加。总之,LMB-100 治疗会引起全身免疫激活。首次对伴随药物相关 CLS 的炎症和免疫变化进行了描述。