Perioperative Medicine and Intensive Care, Karolinska University Hospital, Stockholm, Sweden.
Department of Physiology and Pharmacology, Section for Anaesthesiology and Intensive Care Medicine, Karolinska Institutet, Stockholm, Sweden.
Scand J Trauma Resusc Emerg Med. 2022 Oct 17;30(1):54. doi: 10.1186/s13049-022-01039-9.
Historically, resuscitation in traumatic cardiac arrest (TCA) has been deemed futile. However, recent literature reports improved but varying survival. Current European guidelines emphasise the addressing of reversible aetiologies in TCA and propose that a resuscitative thoracotomy may be performed within 15 min from last sign of life. To improve clinician understanding of which patients benefit from resuscitative efforts we aimed to describe the characteristics and 30-day survival for traumatic cardiac arrest at a Swedish trauma centre with a particular focus on resuscitative thoracotomy.
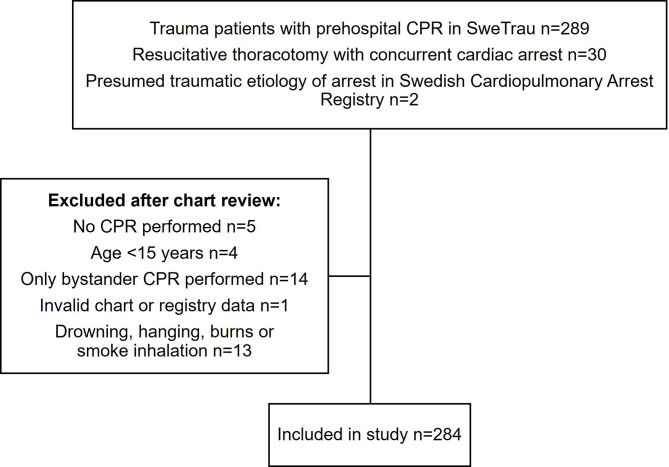
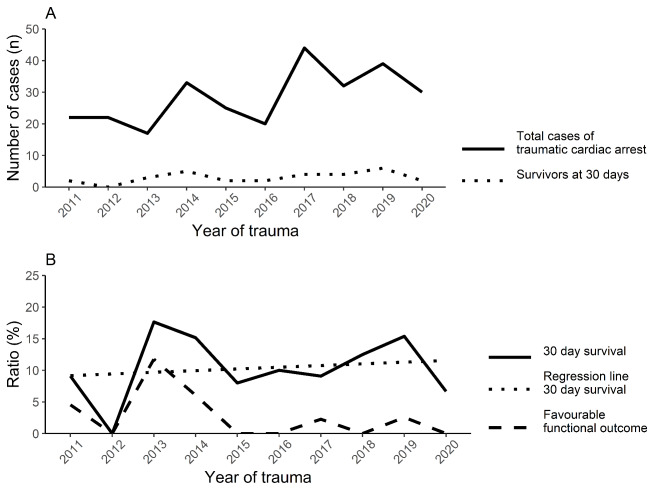
Retrospective cohort study of adult patients (≥ 15 years) with TCA managed at Karolinska University Hospital Solna between 2011 and 2020. Trauma demographics, intra-arrest factors, lab values and procedures were compared between survivors and non-survivors.
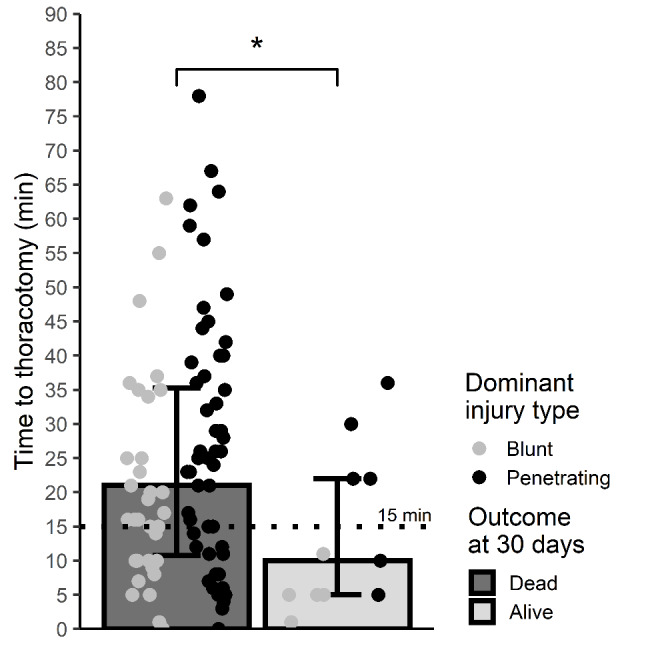
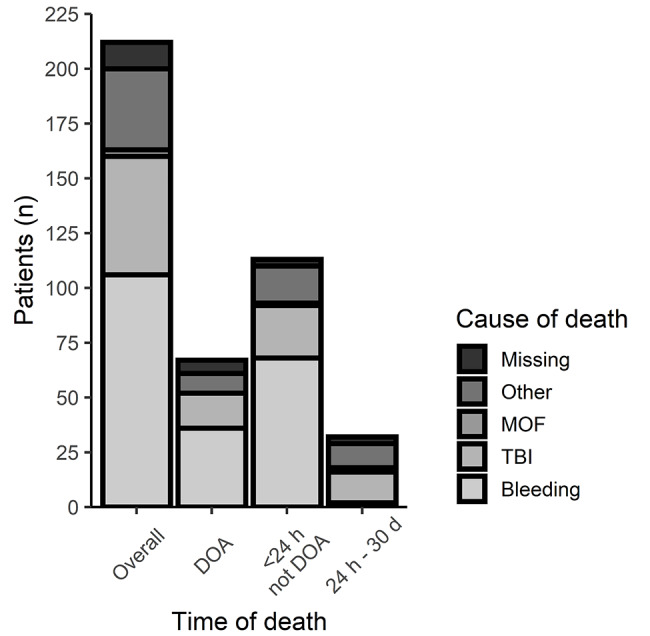
Among the 284 included patients the median age was 38 years, 82.2% were male and 60.5% were previously healthy. Blunt trauma was the dominant injury in 64.8% and median Injury Severity Score (ISS) was 38. For patients with a documented arrest rhythm, asystole was recorded in 39.2%, pulseless electric activity in 24.8% and a shockable rhythm in 6.8%. Thirty patients (10.6%) survived to 30 days with a Glasgow Outcome Scale score of 3 (n = 23) or 4 (n = 7). The most common causes of death were haemorrhagic shock (50.0%) and traumatic brain injury (25.5%). Survivors had a lower ISS (P < 0.001), more often had reactive pupils (P < 0.001) and a shockable rhythm (P = 0.04). In the subset of prehospital TCA, survivors less frequently received adrenaline (epinephrine) (P < 0.001) and in lower amounts (P = 0.02). Of patients that underwent resuscitative thoracotomy (n = 101), survivors (n = 12) had a shorter median time from last sign of life to thoracotomy (P = 0.03), however in four of these survivors the time exceeded 15 min.
Survival after TCA is possible. Determining futility in TCA is difficult and this study demonstrates survivors outside of recent guidelines.
在创伤性心搏骤停(TCA)的复苏中,历史上一直认为复苏是徒劳的。然而,最近的文献报告了存活率的提高,但差异很大。目前的欧洲指南强调了 TCA 中可逆转病因的处理,并提出在最后一次生命体征出现后 15 分钟内可进行抢救性开胸术。为了提高临床医生对哪些患者从复苏努力中受益的理解,我们旨在描述瑞典一家创伤中心 TCA 的特征和 30 天存活率,特别关注抢救性开胸术。
这是一项回顾性队列研究,纳入了 2011 年至 2020 年期间在卡罗林斯卡大学医院索尔纳接受 TCA 治疗的成年患者(≥15 岁)。比较幸存者和非幸存者之间的创伤人口统计学、心搏骤停期间的因素、实验室值和手术。
在 284 名纳入的患者中,中位年龄为 38 岁,82.2%为男性,60.5%之前健康。钝性创伤是主要损伤,占 64.8%,中位损伤严重程度评分(ISS)为 38。对于有记录的停搏节律的患者,记录到心搏骤停 39.2%,无脉电活动 24.8%,可除颤节律 6.8%。30 名患者(10.6%)存活至 30 天,格拉斯哥预后评分 3 分(n=23)或 4 分(n=7)。最常见的死亡原因是出血性休克(50.0%)和创伤性脑损伤(25.5%)。幸存者的 ISS 较低(P<0.001),更常出现有反应的瞳孔(P<0.001)和可除颤节律(P=0.04)。在院前 TCA 的亚组中,幸存者较少接受肾上腺素(epinephrine)(P<0.001)且剂量较低(P=0.02)。接受抢救性开胸术的患者(n=101)中,幸存者(n=12)从最后一次生命体征到开胸术的中位时间较短(P=0.03),但其中 4 例的时间超过 15 分钟。
TCA 后存活是可能的。在 TCA 中确定是否徒劳是困难的,本研究表明幸存者超出了最近的指南。