Pôle de Gynécologie Obstétrique, Médecine Fœtale, Médecine et Biologie de la Reproduction, Centre Olympe de Gouges, CHRU de Tours, Tours, France.
Université de Tours, Tours, France.
PLoS One. 2022 Oct 19;17(10):e0275129. doi: 10.1371/journal.pone.0275129. eCollection 2022.
This trial evaluates whether daily low-dose aspirin initiated before 16 weeks of gestation can reduce preeclampsia and fetal growth restriction in nulliparous women identified by first-trimester uterine artery Dopplers as at high risk of preeclampsia.
This randomized, blinded, placebo-controlled, parallel-group trial took place in 17 French obstetric departments providing antenatal care. Pregnant nulliparous women aged ≥ 18 years with a singleton pregnancy at a gestational age < 16 weeks of gestation with a lowest pulsatility index ≥ 1.7 or a bilateral protodiastolic notching for both uterine arteries on an ultrasound performed between 11+0 and 13+6 weeks by a certified sonographer were randomized at a 1:1 ratio to 160 mg of low-dose aspirin or to placebo to be taken daily from inclusion to their 34th week of gestation. The main outcome was preeclampsia or a birthweight ≤ 5th percentile. Other outcomes included preeclampsia, severe preeclampsia, preterm preeclampsia, preterm delivery before 34 weeks, mode of delivery, type of anesthesia, birthweight ≤ 5th percentile and perinatal death.
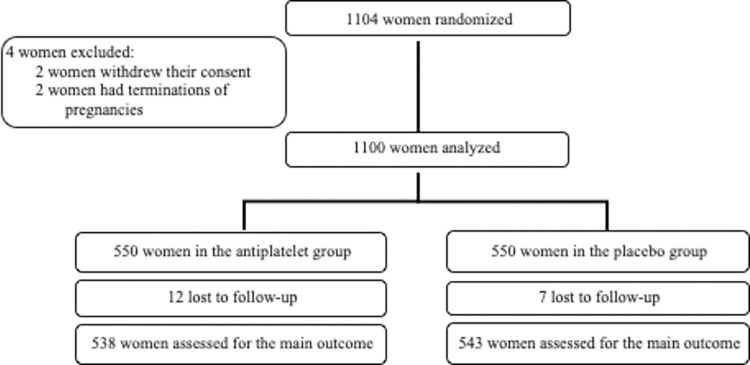
The trial was interrupted due to recruiting difficulties. Between June 2012 and June 2016, 1104 women were randomized, two withdrew consent, and two had terminations of pregnancies. Preeclampsia or a birthweight ≤ 5th percentile occurred in 88 (16.0%) women in the low-dose aspirin group and in 79 (14.4%) in the placebo group (proportion difference 1.6 [-2.6; 5.9] p = 0.45). The two groups did not differ significantly for the secondary outcomes.
Low-dose aspirin was not associated with a lower rate of either preeclampsia or birthweight ≤ 5th percentile in women identified by their first-trimester uterine artery Doppler as at high risk of preeclampsia.
(NCT0172946).
本试验旨在评估在 16 周妊娠前开始每日低剂量阿司匹林是否能降低在妊娠 11+0 至 13+6 周期间由认证超声医师进行的超声检查中双侧子宫动脉舒张末期切迹(notching)的初产妇中通过早孕期子宫动脉多普勒超声检查确定的子痫前期高危人群的子痫前期和胎儿生长受限。
这是一项在 17 个提供产前保健的法国产科部门进行的随机、双盲、安慰剂对照、平行组试验。纳入标准为年龄≥18 岁、单胎妊娠且妊娠<16 周、最低搏动指数≥1.7 或双侧子宫动脉舒张末期切迹(notching)的初产妇,将其随机分配至 160mg 低剂量阿司匹林组或安慰剂组,每日服用,自纳入之日起至第 34 周。主要结局是子痫前期或出生体重<第 5 百分位数。其他结局包括子痫前期、重度子痫前期、早产子痫前期、<34 周早产、分娩方式、麻醉类型、出生体重<第 5 百分位数和围生儿死亡。
由于招募困难,试验被中断。在 2012 年 6 月至 2016 年 6 月期间,共纳入 1104 例患者,其中 2 例退出,2 例终止妊娠。低剂量阿司匹林组和安慰剂组中分别有 88(16.0%)例和 79(14.4%)例发生子痫前期或出生体重<第 5 百分位数(差异 1.6%[-2.6%;5.9%];p=0.45)。两组在次要结局上无显著差异。
对于通过早孕期子宫动脉多普勒超声检查确定的子痫前期高危人群,低剂量阿司匹林并未降低子痫前期或出生体重<第 5 百分位数的发生率。
(NCT0172946)。