Widyaningtiyas Ira, Sarastika Hartono Yudi, Utama Harry Wahyudhy
Department of Radiology, Faculty of Medicine Universitas Airlangga - Dr. Soetomo Academic General Hospital, Surabaya, Indonesia.
Radiol Case Rep. 2022 Oct 12;17(12):4868-4873. doi: 10.1016/j.radcr.2022.09.061. eCollection 2022 Dec.
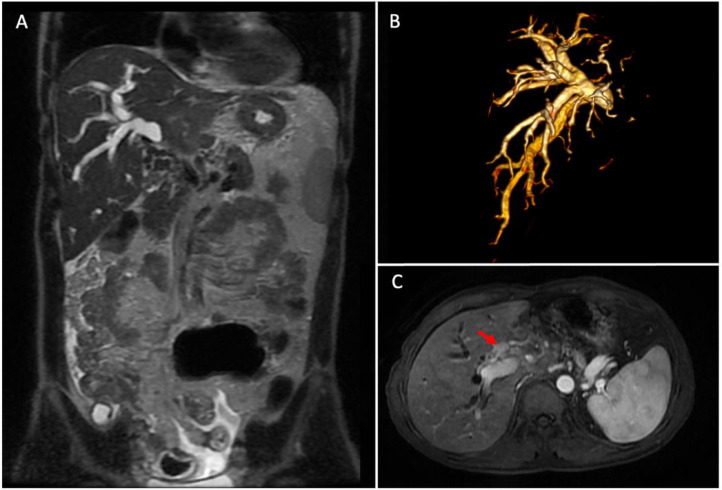
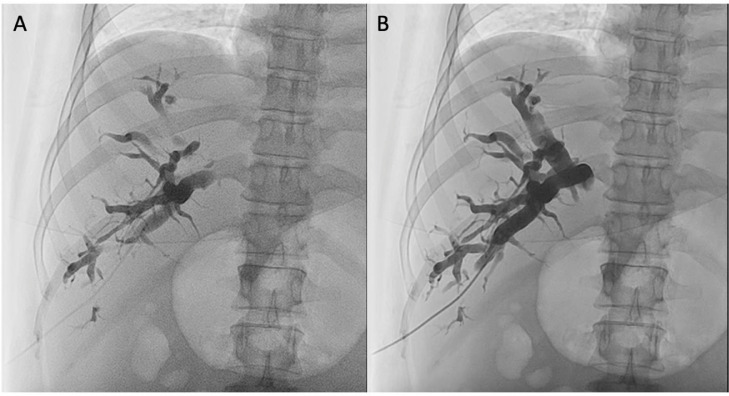
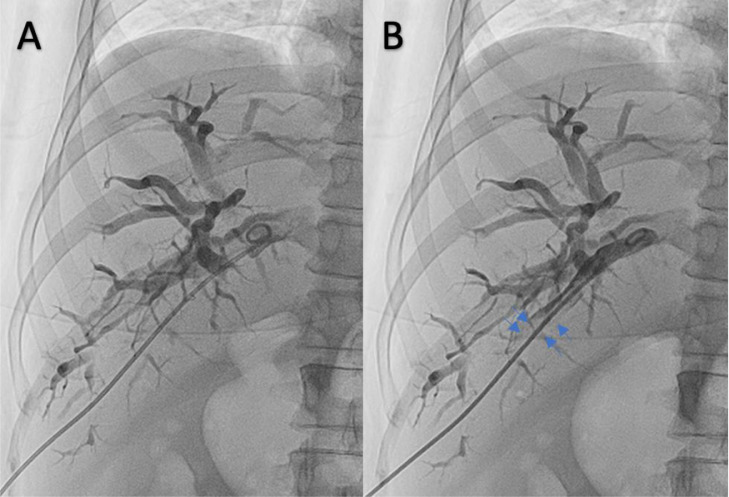
Percutaneous transhepatic biliary drainage (PTBD) is an effective procedure for correcting biliary obstructions. It can be performed under ultrasound and fluoroscopic equipment; however, it may entail serious complications, including bleeding, caused by arterial or venous injury. We present a 49-year-old man presented with a 1-month history of icterus, jaundice, dark urine, and right hypochondrial pain. MR imaging discovered a dilatation of the right intrahepatic bile duct due to obstruction by intrahepatic cholangiocarcinoma. PTBD procedure was performed in the right intrahepatic bile duct. After the pigtail drain device was inserted, the bile fluid color that came out from the pigtail turned sanguineous; nonetheless, the patient's hemodynamic was stable. Therefore, the second cholangiography was performed for evaluation. Some resistance was sensed during contrast injection into the bile duct, and the operator pushed the contrast media a little bit stronger and found a filling defect formed by a clot in the bile duct that suggested high suspicion of vessel injury. Although the patient's hemodynamics was still stable, the operator quickly decided to perform a hepatic arteriography procedure because bright red blood through the tube and a relatively rapid clot formed from the puncture point and distal drain, which were signs of hepatic artery injury. Hepatic arteriography confirmed the location of pseudoaneurysm caused by vessel trauma and arterio-intrahepatic bile duct fistulation. The embolization procedure was performed using PVA-300 into a ruptured hepatic artery branch through a microcatheter. Re-evaluation arteriography showed no pseudoaneurysm or arterio-intrahepatic bile duct fistulation after embolization.
经皮经肝胆道引流术(PTBD)是纠正胆道梗阻的一种有效方法。它可在超声和荧光透视设备下进行;然而,它可能会引发严重并发症,包括因动脉或静脉损伤导致的出血。我们报告一名49岁男性,有1个月的黄疸、深色尿和右季肋部疼痛病史。磁共振成像发现由于肝内胆管癌梗阻导致右肝内胆管扩张。在右肝内胆管进行了PTBD手术。插入猪尾引流装置后,从猪尾流出的胆汁颜色变为血性;尽管如此,患者的血流动力学稳定。因此,进行了第二次胆管造影以进行评估。在向胆管内注入造影剂时感觉到一些阻力,操作人员稍微加大了造影剂的推注力度,发现胆管内有一个由血凝块形成的充盈缺损,高度怀疑有血管损伤。尽管患者的血流动力学仍然稳定,但操作人员迅速决定进行肝动脉造影检查,因为通过导管有鲜红色血液流出,且穿刺点和远端引流处形成了相对较快的血凝块,这些都是肝动脉损伤的迹象。肝动脉造影证实了血管创伤导致的假性动脉瘤的位置以及肝动脉-肝内胆管瘘。通过微导管使用PVA - 300对破裂的肝动脉分支进行了栓塞手术。栓塞后重新评估动脉造影显示无假性动脉瘤或肝动脉-肝内胆管瘘。