Department of Gastroenterology and Hepatology, Odense University Hospital, Odense, Denmark.
Institute for Clinical Research, University of Southern Denmark, Odense, Denmark.
Hepatol Commun. 2022 Dec;6(12):3421-3432. doi: 10.1002/hep4.2075. Epub 2022 Oct 20.
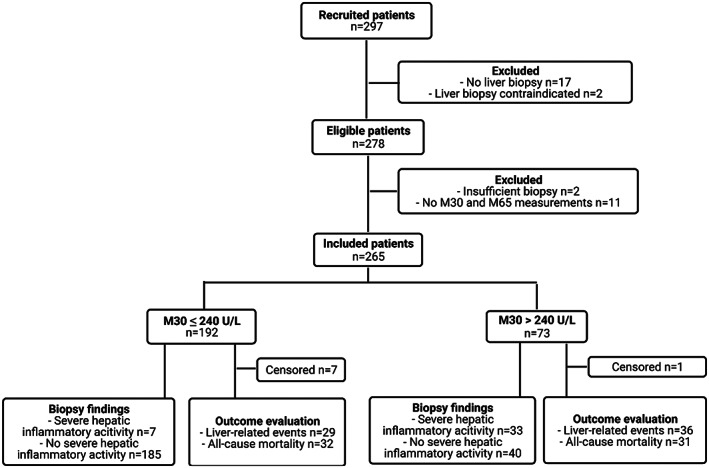
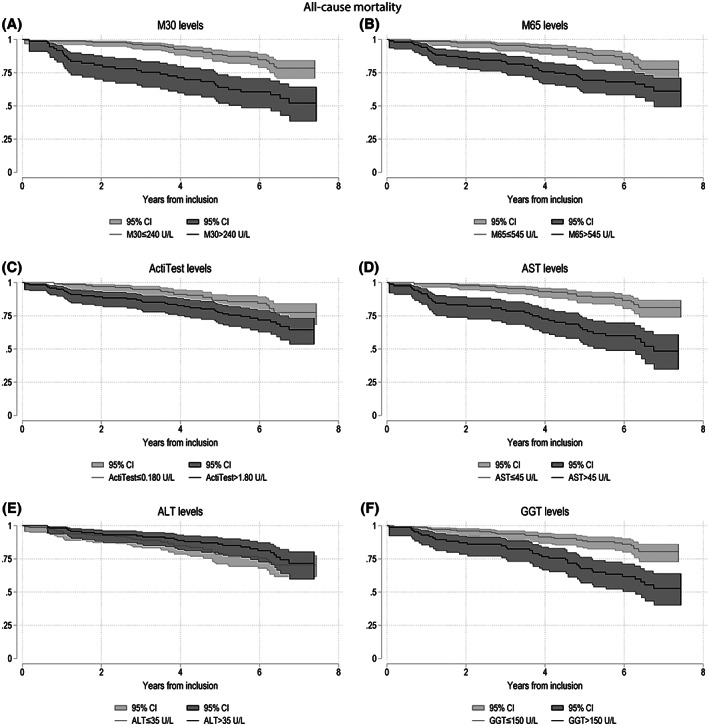
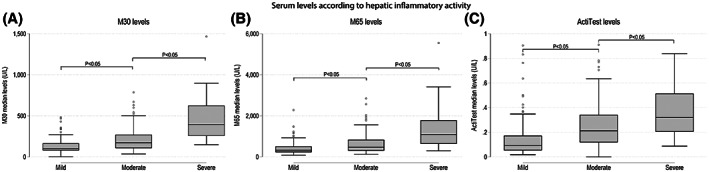
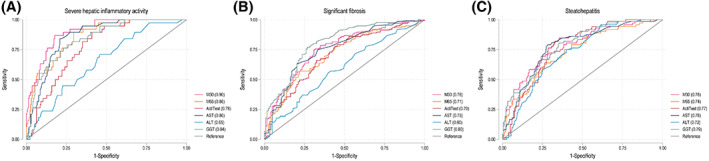
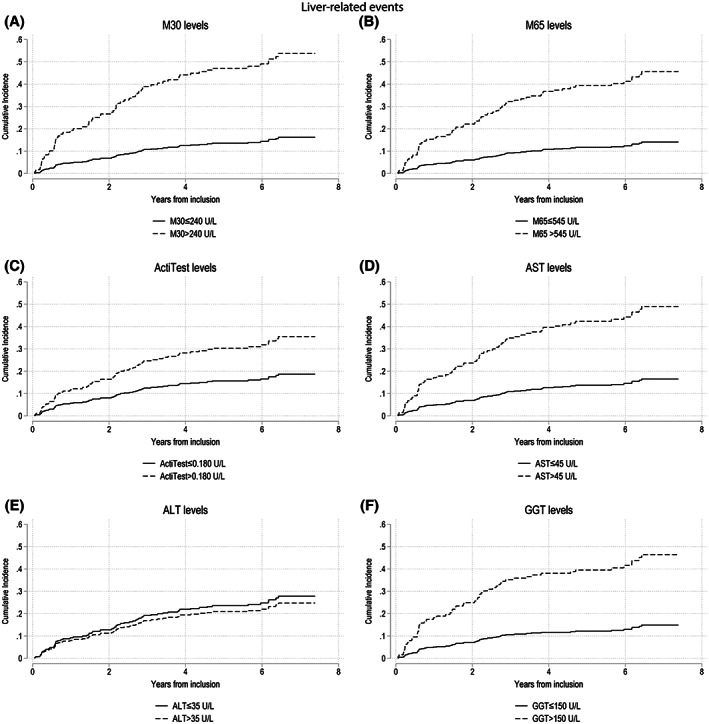
Alcohol-associated liver fibrosis accumulates over decades, driven by hepatic inflammation and cell death. We investigated the diagnostic accuracy of keratin-18 degradation, measured using serum M30 and M65 levels, and the ActiTest for hepatic inflammatory activity in patients with compensated alcohol-associated liver disease (ALD). Furthermore, we evaluated the prognostic accuracy of markers for liver-related events and all-cause mortality. All findings were compared with routine liver function tests: Aspartate aminotransferase (AST), alanine aminotransferase (ALT), and gamma-glutamyltransferase. Our prospective, biopsy-controlled, single-center study included 265 patients with ongoing or prior excessive alcohol intake, representing the full spectrum of compensated ALD. We defined hepatic inflammatory activity as a combined score of lobular inflammation and ballooning. For severe hepatic inflammatory activity (n = 40), we found excellent diagnostic accuracy for M30 (area under the receiver operating characteristics curve [AUROC] = 0.90), M65 (AUROC = 0.86), and AST (AUROC = 0.86). Elevated M30 (M30 > 240 U/L) had the highest positive predictive value (PPV) and specificity, significantly higher than M65, ActiTest and ALT, but not AST (M30: sensitivity = 83%, specificity = 82%, positive predictive value = 45%, negative predictive value = 95%). Patients were followed up for 1445 patient-years. All markers, except for ALT, significantly predicted liver-related events and all-cause mortality. After adjusting for advanced fibrosis, drinking behavior and body mass index, M30 and M65 remained significant predictors of liver-related events, whereas M30 and AST were significant predictors of all-cause mortality. Conclusion: M30 and AST accurately detect severe hepatic inflammatory activity in patients with compensated ALD. M30 was the only significant predictor of both liver-related events and all-cause mortality after adjusting for advanced fibrosis, body mass index, and drinking behavior at inclusion.
酒精相关性肝纤维化在数十年内逐渐积累,其主要由肝炎症和细胞死亡所驱动。我们研究了使用血清 M30 和 M65 水平测量的角蛋白 18 降解,以及 ActiTest 检测代偿性酒精性肝病 (ALD) 患者肝炎症活动的诊断准确性。此外,我们评估了与肝相关事件和全因死亡率相关的标志物的预后准确性。所有发现均与常规肝功能检测(天门冬氨酸氨基转移酶 [AST]、丙氨酸氨基转移酶 [ALT] 和γ-谷氨酰转移酶)进行比较。我们的前瞻性、肝活检对照、单中心研究纳入了 265 例持续或既往过量饮酒的患者,涵盖了代偿性 ALD 的全部范围。我们将肝炎症活动定义为小叶炎症和气球样变性的综合评分。对于严重的肝炎症活动(n=40),我们发现 M30(接受者操作特征曲线下面积 [AUROC] = 0.90)、M65(AUROC = 0.86)和 AST(AUROC = 0.86)具有出色的诊断准确性。M30 升高(M30 > 240 U/L)具有最高的阳性预测值(PPV)和特异性,明显高于 M65、ActiTest 和 ALT,但与 AST 无差异(M30:敏感性=83%,特异性=82%,阳性预测值=45%,阴性预测值=95%)。患者接受了 1445 患者年的随访。所有标志物(ALT 除外)均显著预测与肝相关的事件和全因死亡率。在调整晚期纤维化、饮酒行为和体重指数后,M30 和 M65 仍然是与肝相关事件的显著预测因子,而 M30 和 AST 是全因死亡率的显著预测因子。结论:M30 和 AST 可准确检测代偿性 ALD 患者的严重肝炎症活动。在调整包括晚期纤维化、纳入时的体重指数和饮酒行为在内的因素后,M30 是与肝相关事件和全因死亡率相关的唯一显著预测因子。