Guo Xiaodan, Huang Shaoqing, Shi Yihang, Guan Zhaoming, Chen Sile, Feng Yun, Xia Yanzhe, Zhang Xinhua
Department of Gastrointestinal Surgery, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Department of Pharmacy, The First Affiliated Hospital of Sun Yat-sen University, Guangzhou, China.
Ann Transl Med. 2022 Sep;10(18):1026. doi: 10.21037/atm-22-3746.
Tyrosine kinase inhibitors (TKIs) are currently the main treatment choice for gastrointestinal stromal tumors (GISTs). However, the long-term use of TKIs can lead to drug resistance. There is no study or clinical report of combination therapies of TKIs that have been approved for marketing. Combination pharmacotherapy is a new approach for patients who do not respond to monotherapy. This case provides a reference value for selective combination of TKIs in treating advanced GIST.
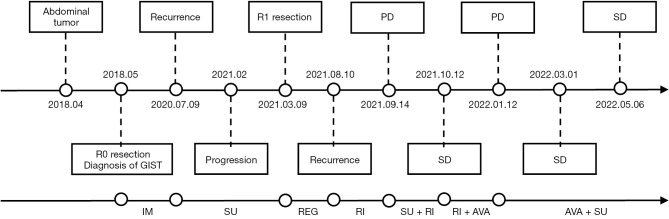
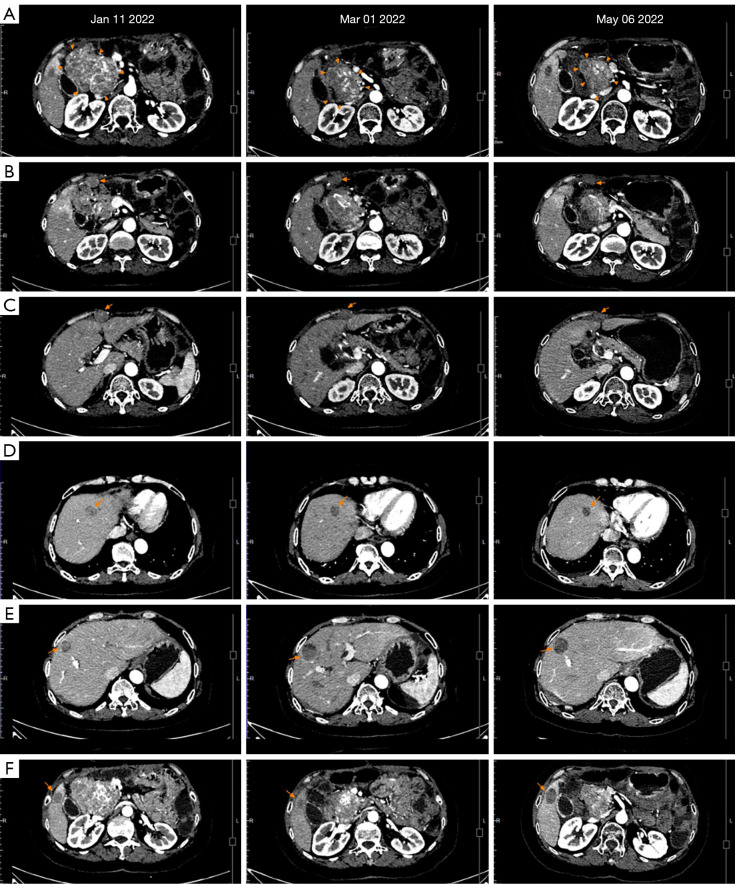
In this article, we report the case of a 55-year-old female who was diagnosed with duodenal GIST in April 2018 and underwent R0 resection. KIT exon 9 mutation was detected. The patient had disease recurrence with multiple abdominal metastases during imatinib adjuvant therapy after 27 months, and failure to 2nd-line sunitinib treatment after 6 months. She underwent a cytoreductive surgery (R1), and the postoperative mutation analysis suggested KIT exon 9 mutation, with newly found secondary KIT_exon16_p. L783V mutation and other mutations on TP53, POT1, and SETD2, etc. The patient experienced short-term tumor control of standard 3rd-line therapy of regorafenib and the rapid progression of the 4th-line of ripretinib afterwards. Different TKI combination therapies (i.e., ripretinib plus sunitinib, ripretinib plus avapritinib and avapritinib plus sunitinib) were administered to the patient sequentially. Ripretinib plus sunitinib led to stable disease but was discontinued due to intolerable adverse effects. Finally, the patient received a combination regimen of avapritinib plus sunitinib. The patient's tumor showed continuous shrinking in 2 consecutive computed tomography scan evaluations within 4 months with acceptable side effects.
Combined type I and type II TKIs of avapritinib combined with sunitinib therapy achieved tumor regression for a heavily multi-line treated patient. Our case provides a reference for a savage treatment choice in refractory GISTs after failure to all standard treatment.
酪氨酸激酶抑制剂(TKIs)是目前胃肠道间质瘤(GISTs)的主要治疗选择。然而,长期使用TKIs会导致耐药。目前尚无已获批上市的TKIs联合疗法的研究或临床报告。联合药物治疗是一种针对单药治疗无效患者的新方法。本病例为晚期GIST患者选择TKIs联合治疗提供了参考价值。
本文报告了一名55岁女性患者的病例,该患者于2018年4月被诊断为十二指肠GIST并接受了R0切除。检测到KIT外显子9突变。患者在接受伊马替尼辅助治疗27个月后出现疾病复发并伴有多处腹部转移,在接受二线舒尼替尼治疗6个月后治疗失败。她接受了减瘤手术(R1),术后突变分析显示为KIT外显子9突变,新发现继发性KIT_exon16_p.L783V突变以及TP53、POT1和SETD2等其他突变。患者接受瑞戈非尼标准三线治疗后肿瘤得到短期控制,但随后四线利培替尼治疗时肿瘤迅速进展。该患者先后接受了不同的TKI联合治疗(即利培替尼加舒尼替尼、利培替尼加阿伐替尼以及阿伐替尼加舒尼替尼)。利培替尼加舒尼替尼使病情稳定,但因无法耐受的不良反应而停药。最后,患者接受了阿伐替尼加舒尼替尼的联合方案。在4个月内的连续2次计算机断层扫描评估中,患者的肿瘤持续缩小,且副作用可接受。
阿伐替尼联合舒尼替尼的I型和II型TKIs联合治疗使一名经过多线治疗的患者肿瘤消退。我们的病例为难治性GIST患者在所有标准治疗失败后提供了一种激进治疗选择的参考。